06/04/2026
2viewsACLF vs ALF: How to Tell Them Apart and Why It Changes Everything About Treatment
ACLF and ALF look similar on admission but require completely different management. Here's how to tell them apart and why it matters
Quick Answer
ACLF and ALF look similar on admission but require completely different management. Here's how to tell them apart and why it matters

A 58-year-old man with known alcohol-related cirrhosis is admitted with jaundice, confusion, and a bilirubin of 18 mg/dL. Three beds down, a 24-year-old woman with no liver history presents with the same triad — jaundice, encephalopathy, bilirubin of 22 mg/dL — after two weeks of paracetamol overuse. Both patients look critically unwell. Both will be labelled "liver failure" in the initial clerking note. But the diagnosis, prognosis, and management for these two patients are so fundamentally different that conflating them is one of the more consequential errors in hepatology.
The distinction between acute-on-chronic liver failure and acute liver failure matters not just academically but at every decision point: who gets admitted to the ICU, who gets listed for transplant, which vasopressors are appropriate, how long you wait before escalating. The challenge is that on a busy admissions ward, the two can look identical for the first few hours. Both present with jaundice, encephalopathy, and coagulopathy. Both can deteriorate within 24 hours. And the underlying liver disease in ACLF may never have been formally diagnosed before. This post is specifically about the diagnostic framework that separates them — and what changes downstream once you get it right.
The Defining Difference: Underlying Liver Architecture
The single most important question to answer is whether the liver that has failed was previously normal or previously diseased. That question determines everything else.
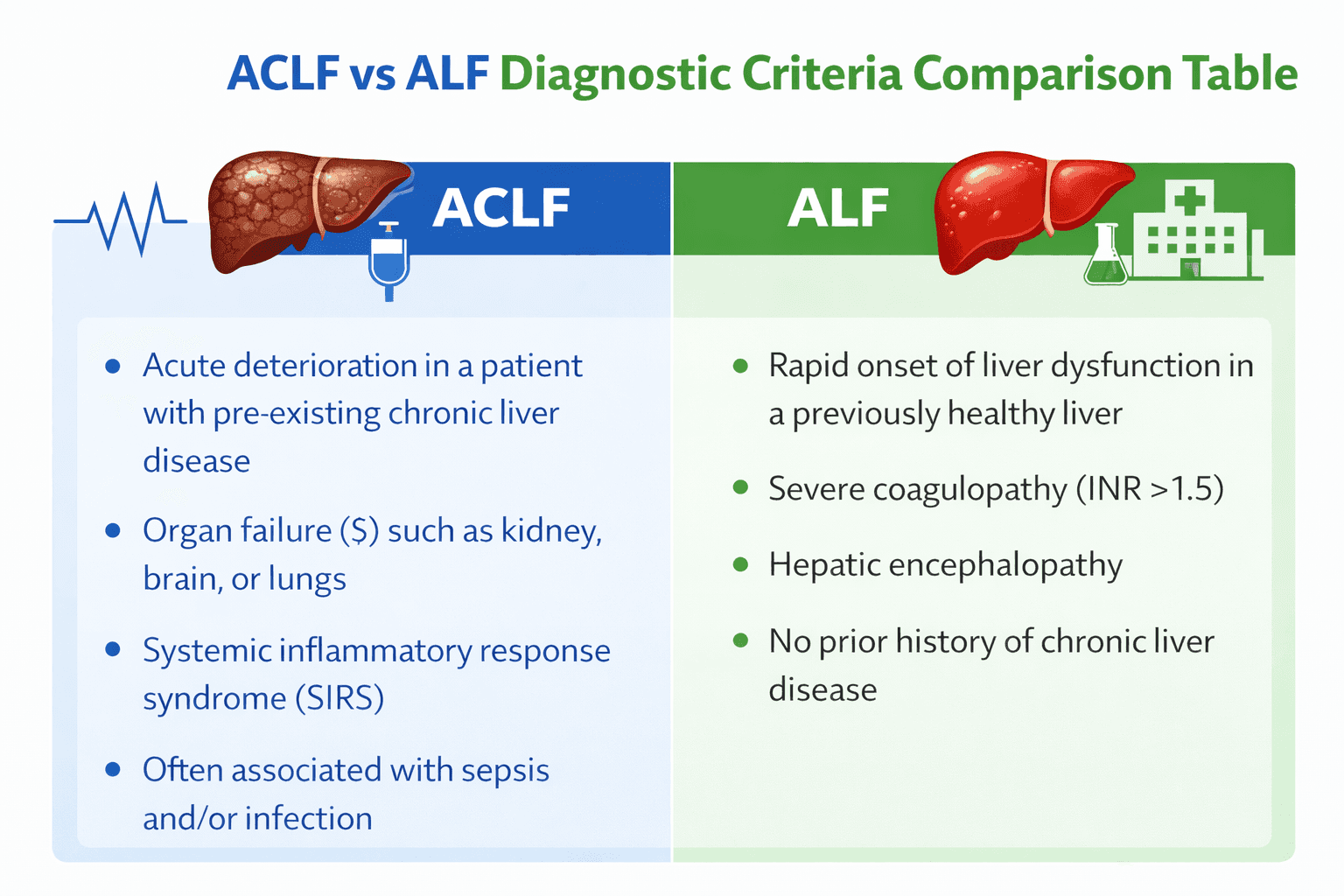
Acute liver failure, as defined by the American Association for the Study of Liver Diseases (AASLD), is the development of coagulopathy (INR ≥1.5) and encephalopathy within 26 weeks in a patient without pre-existing liver disease. The pathophysiology is a sudden, catastrophic hepatocyte loss — from paracetamol toxicity, viral hepatitis A or E, autoimmune hepatitis, Wilson's disease, or ischaemia — in a liver with normal architecture and no fibrosis. The key implication: this liver has full regenerative potential. If the insult is removed and the patient is supported through the acute phase, spontaneous recovery is possible. This is why the transplant decision in ALF is time-limited and reversible — the listing criteria are designed to identify those who will not recover spontaneously, not those who can never regenerate.
ACLF is a different beast. Defined by the EASL-CLIF consortium criteria from the landmark CANONIC study, ACLF requires an acute decompensation event — infection, alcohol-related hepatitis, GI bleeding, or an unknown precipitant — superimposed on chronic liver disease, with evidence of organ failure by the EASL-CLIF criteria (renal, hepatic, cerebral, coagulation, circulatory, or respiratory). The underlying liver has already lost architectural integrity. There is no regenerative reservoir. The acute decompensation tips a compensated or previously decompensated cirrhotic into a state of systemic inflammation and multi-organ failure that carries a 28-day mortality of 30–40% in ACLF grade 2, and over 60% in grade 3.
Clinical scenario
A 47-year-old man presented to the emergency department with a three-day history of increasing jaundice, abdominal distension, and confusion. His family reported he had been drinking heavily for 20 years but had never been formally diagnosed with liver disease. On examination: encephalopathy grade II, bilateral asterixis, tense ascites, spider naevi, palmar erythema. INR 2.8, bilirubin 24 mg/dL, creatinine 2.1 mg/dL, sodium 128 mEq/L. No history of paracetamol use. No recent travel.
The clinical picture pointed immediately to ACLF, not ALF — the stigmata of chronic liver disease alone disqualified an ALF diagnosis. The precipitant was identified as an alcohol binge superimposed on compensated cirrhosis. He was graded ACLF-2 by EASL-CLIF criteria (renal and hepatic organ failure). The management priority shifted immediately: not spontaneous recovery, but aggressive precipitant treatment, infection surveillance, and hepatology review for transplant candidacy assessment. He was not listed under ALF criteria — he was evaluated under the ACLF-specific transplant pathway, which has fundamentally different timing and reversibility assumptions.
Why the ACLF vs ALF Distinction Drives Completely Different Treatment Decisions
Once you have the correct diagnosis, three management decisions diverge immediately.
Transplant listing pathway. In ALF, listing is urgent and time-sensitive — King's College Criteria or Clichy criteria guide the decision, and the window for listing can close within 48–72 hours as cerebral oedema develops. In ACLF, the transplant consideration is different: ACLF-3 carries such high 28-day mortality that early transplantation is increasingly supported by evidence, but the patient must first survive the precipitant treatment window. Per the 2023 EASL guidelines on ACLF, patients with ACLF-3 who survive 3–7 days of intensive management should be urgently evaluated for transplant — the listing decision is not immediate but has a defined reassessment window.
Precipitant identification and treatment. In ALF, the precipitant is usually known or quickly apparent — paracetamol levels, viral serology, autoimmune panel, Wilson's screen. In ACLF, the precipitant search is broader and the stakes of missing it are higher: 30–40% of ACLF cases are precipitated by bacterial infection, and a significant proportion of those infections are spontaneous bacterial peritonitis with no overt clinical signs. Diagnostic paracentesis is mandatory in any ACLF patient with ascites — not optional, not deferred.
Renal management. Hepatorenal syndrome-AKI (HRS-AKI) behaves differently in ACLF versus decompensated cirrhosis without ACLF. Terlipressin response rates are lower, and dose escalation thresholds should be reviewed at 48 hours, not 96 hours. Renal replacement therapy decisions in ACLF-3 need to account for the fact that renal recovery is less likely without transplant.
A frequently overlooked point: the "no prior diagnosis" trap in ACLF
The most common error in differentiating ACLF from ALF is assuming that a patient cannot have ACLF because they have no prior liver diagnosis. This is wrong, and consequential. In the CANONIC study, a significant proportion of ACLF patients had compensated cirrhosis that had never been clinically identified. The presence of physical stigmata — spider naevi, palmar erythema, gynaecomastia, Dupuytren's contracture, parotid enlargement — combined with a platelet count below 150,000/µL and a low albumin should raise immediate suspicion for underlying chronic disease. A single ultrasound showing a nodular liver surface closes the argument. If there is any doubt, managing the patient as ACLF is the safer default — the consequence of under-treating ACLF as ALF (waiting for spontaneous recovery that cannot come) is far more dangerous than the reverse.
Bottom line for clinical practice
The first question at any liver failure presentation is not "how bad is it?" — it is "was the liver previously normal?" Stigmata of chronic disease, low platelets, and low albumin answer this before any biopsy or imaging.
ACLF grade is determined by the number of organ failures using EASL-CLIF criteria — not by bilirubin level alone. Grade 3 (three or more organ failures) carries >60% 28-day mortality and demands immediate transplant evaluation.
In any ACLF patient with ascites, diagnostic paracentesis is mandatory on admission — bacterial infection precipitates 30–40% of ACLF episodes, often silently.
Do not apply King's College Criteria to an ACLF patient — they were derived from ALF populations and are not validated for chronic liver disease backgrounds.
Terlipressin response in ACLF-related HRS-AKI should be formally reassessed at 48 hours, not the standard 96-hour window used in non-ACLF settings.
The next time you admit a patient with jaundice and encephalopathy, GastroAGI can walk you through the ACLF vs ALF differentiation in real time — enter the clinical details and get a structured, guideline-anchored assessment of diagnosis, grade, precipitant checklist, and next steps within seconds.
Use GastroAGI For Free.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.