08/07/2026
316viewsACG 2026 Diverticulitis Guideline: CT Confirmation, Selective Antibiotics, and Smarter Follow-Up
ACG’s 2026 diverticulitis guideline emphasizes CT confirmation, selective antibiotics, tailored colonoscopy, and lifestyle prevention.
Quick Answer
ACG’s 2026 diverticulitis guideline emphasizes CT confirmation, selective antibiotics, tailored colonoscopy, and lifestyle prevention.
Introduction
Diverticulitis remains one of the most common reasons patients present with acute lower abdominal pain, outpatient GI consultation, emergency department visits, antibiotic exposure, colonoscopy referrals, and surgical discussions. Yet the management of diverticulitis has changed substantially over the past decade.
The American College of Gastroenterology has now listed its July 2026 ACG Clinical Guideline on Colonic Diverticulitis, authored by Anne Peery, MD, MSCR, and colleagues. The guideline is available through the ACG guideline portal, with an accompanying highlights document summarizing key clinical recommendations.
The most important message is that diverticulitis management is becoming more individualized. The update reinforces CT-based confirmation at first presentation, selective use of colonoscopy, selective rather than routine antibiotics in carefully chosen uncomplicated cases, and prevention strategies focused on diet, NSAID avoidance, weight management, physical activity, alcohol moderation, and smoking cessation.
For GastroAGI readers, this is a highly practical guideline because it speaks directly to day-to-day decisions: Who needs CT? Who can avoid antibiotics? Who needs colonoscopy? When should surgery be discussed? And what advice should patients receive after recovery?
Why this update matters
Historically, diverticulitis was often treated as a uniform condition: diagnose clinically, prescribe antibiotics, recommend dietary restrictions, and consider colonoscopy after recovery. The newer approach is more nuanced.
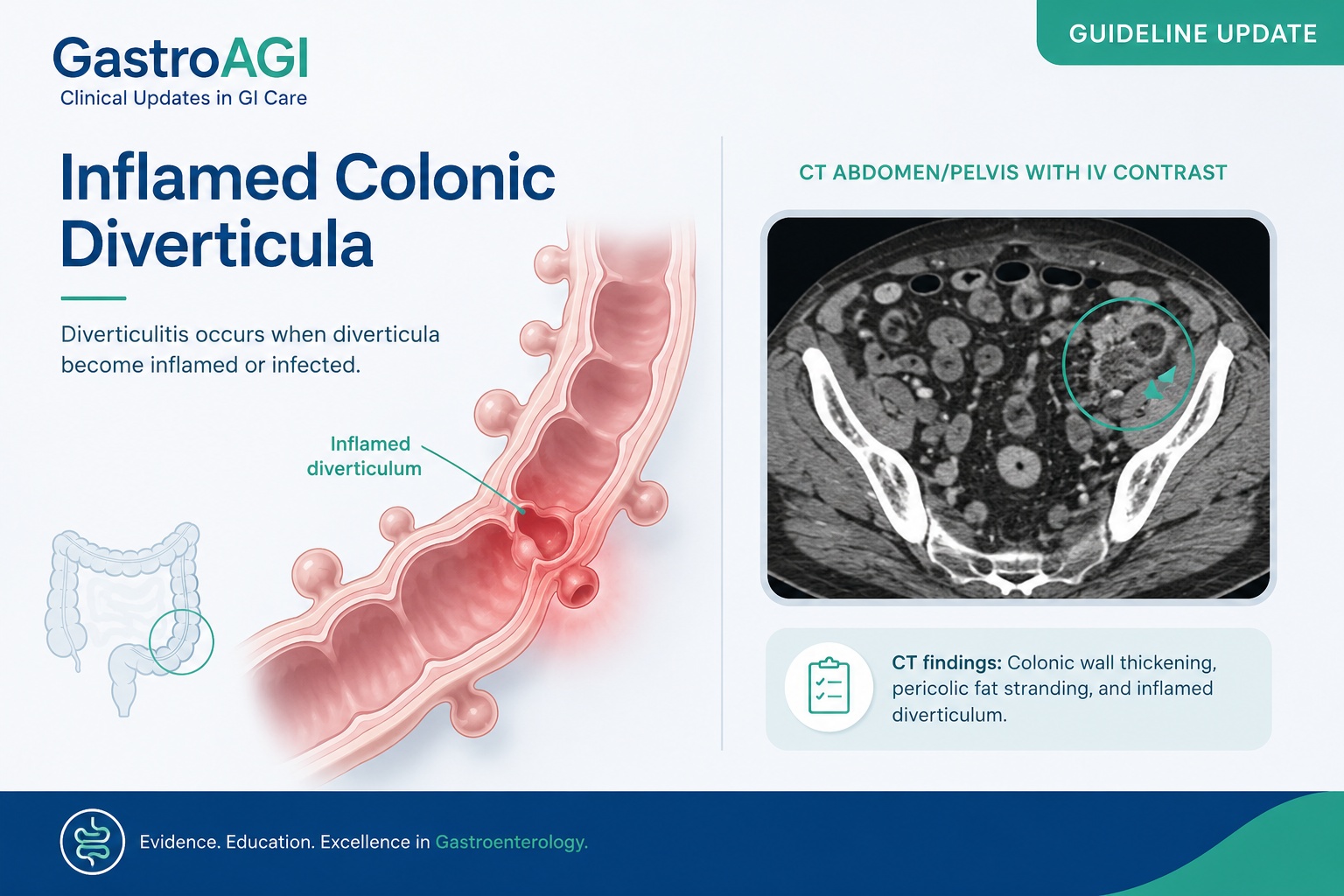
The ACG highlights document emphasizes that clinical evaluation alone is often inaccurate, and recommends CT at first presentation to confirm diverticulitis, rule out alternative diagnoses, assess severity, and localize disease.
This matters because left lower quadrant pain is not always diverticulitis. Alternative diagnoses may include colorectal cancer, ischemic colitis, inflammatory bowel disease, gynecologic pathology, urinary tract disease, appendicitis in atypical anatomy, or other intra-abdominal inflammatory processes. A CT-confirmed diagnosis also helps distinguish uncomplicated disease from abscess, perforation, phlegmon, stricture, or fistula.
The guideline also reframes antibiotic use. According to the ACG highlights, acute uncomplicated diverticulitis can be managed without antibiotics in selected patients who are immunocompetent, hemodynamically stable, outpatient, able to tolerate oral intake, without SIRS or complicated disease, not medically frail, and able to follow up reliably.
That is a clinically important shift. It supports antibiotic stewardship while preserving safety by identifying higher-risk groups who still warrant antimicrobial therapy.
What the guideline found
The ACG highlights divide diverticulitis into clinically meaningful phenotypes: uncomplicated diverticulitis, chronic or smoldering diverticulitis, and complicated diverticulitis. Uncomplicated diverticulitis is described as localized inflammation of diverticula without abscess, perforation, stricture, or fistula. Chronic or smoldering diverticulitis refers to inflammation that persists for weeks to months, often with partial or complete symptomatic improvement followed by relapse after antibiotics are stopped. Complicated diverticulitis includes inflammation with phlegmon, abscess, or perforation, with strictures and fistulas as possible delayed complications.
For diagnosis, the key recommendation is CT confirmation at first presentation. This is intended to confirm the diagnosis, exclude mimics, determine severity, and localize the involved segment.
For natural history, the ACG highlights note that the risk of complicated diverticulitis is highest with the first episode and decreases with recurrences. The document lists recurrence risk as approximately 22% after a first episode and 55% after a second episode, with high recurrence risk after three or more episodes.
For colonoscopy, the guideline distinguishes complicated from uncomplicated disease. After complicated diverticulitis, colonoscopy is recommended to rule out missed cancer or premalignant lesions. After uncomplicated diverticulitis, colonoscopy is recommended only when alarm symptoms are present or the patient is not up to date with colorectal cancer screening. Alarm symptoms listed in the ACG highlights include unintentional weight loss, change in bowel habits, iron-deficiency anemia, bloody stools, and persistent abdominal pain.
For antibiotics, the guideline supports non-antibiotic management in carefully selected uncomplicated cases. Antibiotics are advised for patients who are immunocompromised, frail, medically complex, unable to tolerate oral intake, worsening clinically, have markedly elevated inflammatory markers or higher-risk imaging features, or lack reliable follow-up or support.
For prevention, the ACG highlights recommend a high-fiber, plant-forward diet; advise against routinely avoiding nuts, seeds, corn, or popcorn; recommend avoiding regular NSAID use when possible; and support alcohol moderation, weight loss when overweight or obese, regular physical activity, and smoking cessation.
Clinical interpretation
The 2026 ACG guidance reflects a broader movement in diverticulitis care: away from reflexive treatment and toward risk-stratified management.
First, CT confirmation is not simply a diagnostic formality. It is the foundation for safe decision-making. A patient with uncomplicated sigmoid diverticulitis, no systemic inflammatory response, good oral intake, and reliable follow-up is very different from a patient with a contained perforation, abscess, immunosuppression, or clinical deterioration.
Second, the antibiotic recommendation should not be misread as “antibiotics are unnecessary.” The guideline’s message is more precise: antibiotics can be avoided in selected low-risk uncomplicated cases, but they remain appropriate in higher-risk patients. This is an important distinction for patient counseling and for avoiding undertreatment in vulnerable groups.
Third, colonoscopy after diverticulitis should be individualized. The guideline supports colonoscopy after complicated disease because of concern for missed malignancy or premalignant lesions. In uncomplicated disease, however, routine colonoscopy is not required if the patient has no alarm symptoms and is already current with colorectal cancer screening.
Fourth, the prevention section is clinically useful because many patients still believe they must avoid seeds, nuts, popcorn, or corn after diverticulitis. The ACG highlights specifically state that these foods do not need to be routinely avoided.
Practical implications for gastroenterologists
For GI clinicians, this guideline can be translated into a practical framework.
At first presentation, confirm the diagnosis with CT when appropriate, especially if the patient has not previously had imaging-confirmed diverticulitis. This helps avoid anchoring on a clinical diagnosis when another condition may be present.
After CT, classify the episode as uncomplicated, chronic or smoldering, or complicated. This classification should drive treatment intensity, follow-up, and referral decisions.
For uncomplicated diverticulitis, assess whether the patient is low risk enough for observation without antibiotics. Key safety checks include immune status, hemodynamic stability, oral intake, absence of SIRS, absence of complicated disease, frailty, comorbidity burden, and ability to follow up.
For colonoscopy planning, avoid automatic post-diverticulitis colonoscopy in every uncomplicated case. Instead, ask whether the patient had complicated disease, has alarm symptoms, or is overdue for colorectal cancer screening.
For recurrent disease, the guideline supports referral for surgical discussion when recurrent uncomplicated diverticulitis meaningfully affects quality of life. Importantly, elective resection may lower recurrence risk, but it does not eliminate recurrence.
For prevention counseling, move away from outdated food restrictions and toward sustainable lifestyle advice: high-fiber plant-forward diet, avoiding regular NSAIDs when possible, weight management, activity, alcohol moderation, and smoking cessation.
Limitations and caution
This guideline is clinically important, but it does not remove the need for judgment.
Non-antibiotic management is not appropriate for every patient with uncomplicated diverticulitis. The ACG highlights define specific features that support antibiotic use, including immunocompromise, frailty, medical complexity, poor oral intake, worsening clinical status, high inflammatory burden or concerning imaging, and unreliable follow-up.
Similarly, avoiding routine colonoscopy after uncomplicated diverticulitis applies only when there are no alarm symptoms and the patient is already current with colorectal cancer screening. Persistent pain, bleeding, iron-deficiency anemia, change in bowel habits, or weight loss should prompt further evaluation.
The prevention recommendations are also not a guarantee against recurrence. They are risk-reduction strategies, not definitive preventive therapy.
GastroAGI takeaway
The 2026 ACG diverticulitis guideline gives gastroenterologists a practical, risk-stratified approach to a common clinical problem.
The key shifts are clear: confirm first presentations with CT, avoid routine antibiotics in carefully selected low-risk uncomplicated cases, reserve colonoscopy after uncomplicated disease for patients with alarm symptoms or incomplete colorectal cancer screening, and counsel patients using evidence-aligned prevention advice rather than outdated dietary restrictions.
For daily practice, the central message is not less care. It is smarter care: accurate diagnosis, selective treatment, individualized follow-up, and prevention counseling that patients can realistically follow.
Reference / Source
American College of Gastroenterology. Colonic Diverticulitis – Guideline. July 2026. ACG guideline portal and ACG guideline highlights document.
Key Points
ACG lists the Colonic Diverticulitis Guideline as a July 2026 guideline update.
Clinical evaluation alone is often inaccurate; CT is recommended at first presentation to confirm diagnosis and assess severity.
Selected low-risk patients with acute uncomplicated diverticulitis may be managed without antibiotics.
Antibiotics remain appropriate for immunocompromised, frail, medically complex, clinically worsening, or higher-risk patients.
Colonoscopy is recommended after complicated diverticulitis, but not routinely after uncomplicated disease unless alarm symptoms are present or CRC screening is not up to date.
Patients do not need to routinely avoid nuts, seeds, corn, or popcorn.
Prevention counseling should emphasize a high-fiber plant-forward diet, physical activity, smoking cessation, alcohol moderation, weight management, and avoiding regular NSAID use when possible.
Explore GastroAGI
If you are a gastroenterologist, trainee, researcher, or medical educator navigating journals, guidelines, conferences, and clinical questions every day, GastroAGI is built for you.
GastroAGI brings GI-focused intelligence into one structured platform — helping users learn, reason, and communicate with more clarity across Student, Clinician, and Patient modes.
Explore how specialized AI can support modern gastroenterology workflows.
Visit GastroAGI: https://gastroagi.com
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.