15/06/2026
26viewsAnti-IL-10 Autoantibodies in IBD: What the 2026 NEJM Study Means for How You Classify and Treat Your Patients
A new NEJM study identifies anti-IL-10 neutralizing autoantibodies in 3.5% of IBD patients and none in healthy controls - a targetable disease subtype.
Quick Answer
A new NEJM study identifies anti-IL-10 neutralizing autoantibodies in 3. 5% of IBD patients and none in healthy controls - a targetable disease subtype.
A 34-year-old woman with longstanding ulcerative colitis fails successive trials of mesalazine, azathioprine, and two biologics. Her disease remains active, her fecal calprotectin sits persistently above 1,000 μg/g, and her colonoscopy looks like she never had treatment. The standard algorithm has run out of moves. The 2026 NEJM study on anti–IL-10 autoantibodies may explain why - and what to do next.
IBD has always been treated as two diseases (Crohn's disease and ulcerative colitis) shaped by environment, microbiome, and polygenic susceptibility. What the new NEJM paper makes clear is that a clinically meaningful subset of patients carries a third driver: functional autoimmunity against interleukin-10, the gut's primary immunosuppressive cytokine. These patients are phenotypically indistinguishable from conventional IBD by endoscopy or histology, but they are mechanistically distinct - and they may require a fundamentally different therapeutic approach. For the clinician managing a refractory case, this is not academic. The distinction has direct treatment implications that conventional IBD workup will never surface.
How Anti–IL-10 Autoantibodies Produce an IBD Phenotype
IL-10 functions as the intestinal immune system's brake. It suppresses pro-inflammatory cytokine production, particularly TNF, IL-23, and IL-1β, and maintains mucosal homeostasis. Biallelic loss-of-function mutations in IL10, IL10RA, or IL10RB produce a well-characterized syndrome of severe, fistulizing, early-onset colitis - a monogenic IBD phenocopy. The 2024 NEJM case series by Griffin et al. first described that the same phenotype could be generated not by genetic deletion but by high-titer neutralizing autoantibodies against IL-10 in two children with very early onset IBD. In one case, B-cell depletion therapy reduced autoantibody titers and allowed complete withdrawal of conventional IBD therapy.
The 2026 large-cohort NEJM paper now scales this finding to a population level. Across 4,909 patients with IBD drawn from the Oxford cohort and the UK IBD BioResource, neutralizing anti–IL-10 autoantibodies were detected in 173 patients - a prevalence of 3.5% (95% CI, 3.0–4.1). Critically, zero of the 1,006 healthy controls tested positive (P<0.001). This is not a noisy biomarker. The 100% specificity in controls establishes that anti–IL-10 seropositivity is biologically meaningful, not background noise. Functionally, high anti–IL-10 activity in serum correlated with reduced detectable IL-10 and an exaggerated pro-inflammatory cytokine release - exactly what would be expected if endogenous IL-10 signaling were being blocked in real time.
The HLA-DRB1*01:03 Connection: A Genetic Risk Factor You Can Test For
Anti–IL-10 seropositivity was not randomly distributed across the cohort. It was strongly and consistently associated with carriage of the HLA-DRB1*01:03 allele - the same allele already recognized as the strongest genetic risk factor for severe ulcerative colitis. Across two independent cohorts and three analytical methods (imputed data in the Oxford cohort: OR 50.0, 95% CI 16.4–152.3; UK IBD BioResource: OR 24.7, 95% CI 14.5–42.1; high-resolution sequencing: OR 29.5, 95% CI 12.2–71.1), the association held at striking magnitude and statistical confidence. Oxford researchers first identified the HLA-DRB1*01:03 - severe UC link three decades ago; the 2026 paper finally provides a credible mechanistic explanation for it.
Clinically, this matters because HLA-DRB1*01:03 genotyping is a real, available test. It is not routine in IBD practice, but it is accessible. For a patient with refractory IBD, particularly early-onset or unexpectedly aggressive disease, knowing that HLA-DRB1*01:03 carriage confers an odds ratio of approximately 25–50 for anti–IL-10 seropositivity changes how you think about the diagnostic workup. A positive HLA-DRB1*01:03 result substantially raises pre-test probability for this subtype, making anti–IL-10 antibody testing the next logical step.
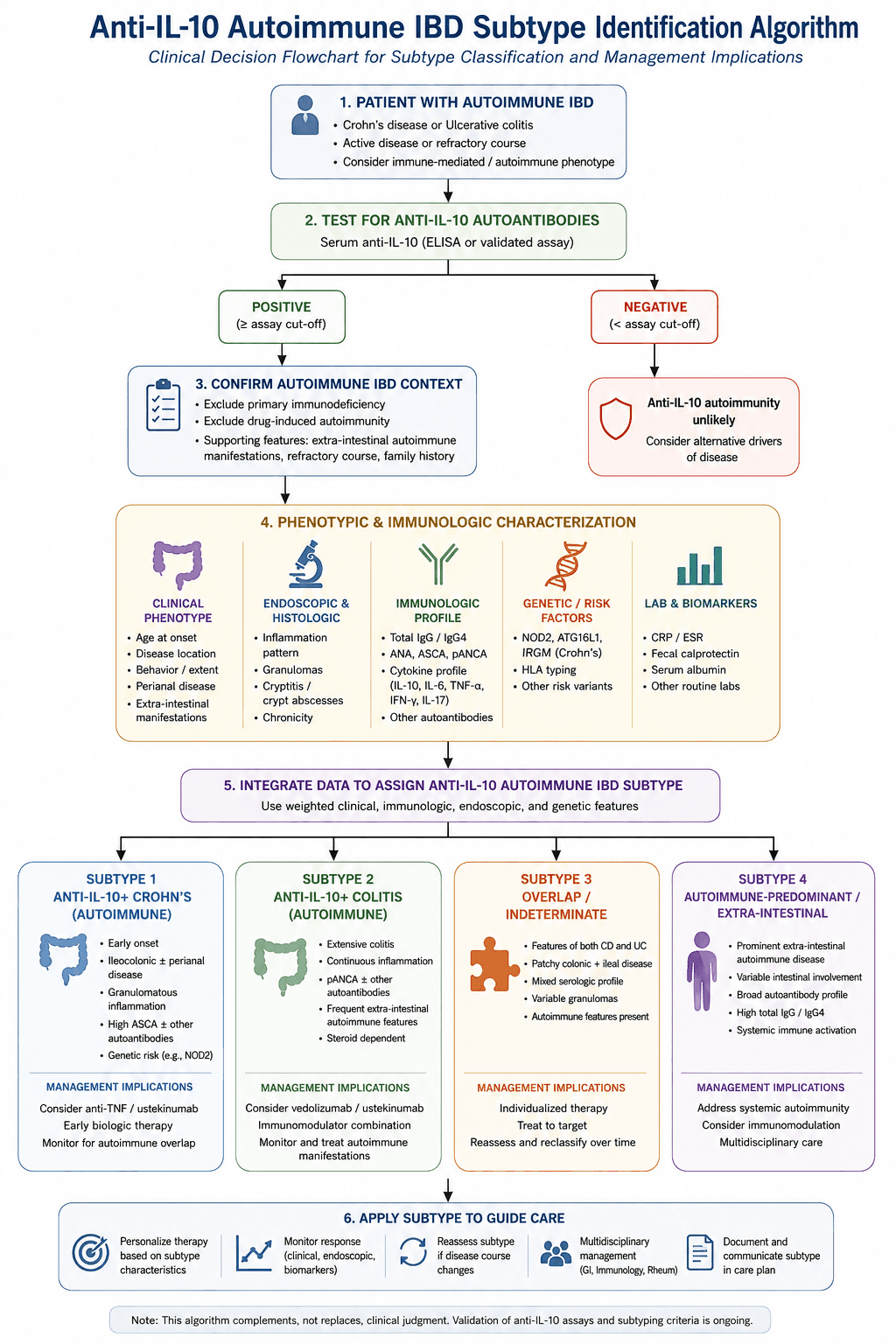
This also spans disease phenotype. The 3.5% seropositive group included both Crohn's disease and ulcerative colitis patients - meaning anti–IL-10 autoimmunity does not respect the endoscopic categories gastroenterologists rely on to classify disease. Some patients currently labeled UC or CD may need to be reclassified, at least mechanistically.
Clinical Scenario: When the Biologic History Does Not Add Up
A 28-year-old male with a diagnosis of Crohn's disease at age 19 had responded partially to infliximab for two years before losing response. He was switched to vedolizumab with minimal improvement, then ustekinumab with persistent CRP elevation and ongoing symptoms despite apparent mucosal healing on MRI enterography. His physician was preparing to escalate to a combination strategy or clinical trial referral.
On closer review, his disease had been unusually refractory from the outset - initial presentation was severe, requiring early steroid escalation, and he had never achieved steroid-free remission for more than four months. HLA genotyping returned HLA-DRB1*01:03 positive. Anti–IL-10 autoantibody testing confirmed high-titer seropositivity with functional neutralization confirmed by cytokine-release bioassay. The working diagnosis shifted: this was not refractory Crohn's disease, but anti–IL-10 autoimmune IBD - a mechanistically distinct entity. A B-cell depletion strategy is now under discussion, consistent with the 2024 NEJM case precedent in which rituximab-driven decline in autoantibody titer allowed withdrawal of conventional IBD therapy altogether.
Implications for Refractory IBD: Moving Toward Targeted B-Cell Depletion
Current IBD treatment operates on the assumption that all patients share the same underlying immune dysregulation - and adjusts biologic target accordingly. TNF inhibitors, anti-integrin therapy, IL-12/23 blockade, and JAK inhibitors all downstream-suppress inflammation without addressing the upstream mechanism in anti–IL-10 seropositive patients. Blocking TNF in a patient whose problem is neutralization of IL-10 is treating the symptom of a fire, not the fuel.
The proof-of-concept for mechanism-specific treatment comes from the 2024 Griffin et al. case series. In Patient 1, B-cell depletion with rituximab caused a sustained decline in anti–IL-10 titer. As autoantibodies disappeared, intestinal inflammation resolved, and conventional IBD therapy was ultimately withdrawn - an outcome essentially unheard of in longstanding IBD without surgical resection. Patient 2, with lower-titer antibodies, had a milder course managed without B-cell depletion, suggesting that severity tracks with antibody titer and that not all seropositive patients require the same intensity of intervention.
What the 2026 cohort paper adds is epidemiological plausibility: 3.5% of IBD patients is not a rarity. Extrapolated to the UK alone, this represents an estimated 15,000–20,000 people. At a national level - or across any large IBD center - these patients exist in the practice now.

A Frequently Overlooked Point: This Is Not Just a Pediatric Finding
The original 2024 case series involved children with very early onset IBD, which led some readers to bracket this as a pediatric curiosity. The 2026 cohort study clarifies that anti–IL-10 seropositivity occurs across adult IBD populations - both Crohn's disease and ulcerative colitis, in adult cohorts sampled from tertiary IBD centers. Very early onset disease may represent the most phenotypically dramatic end of the spectrum, but the mechanism is not age-restricted. Adult patients with unexplained biologic non-response should be considered for anti–IL-10 antibody testing, particularly those who carry HLA-DRB1*01:03 or whose disease progression never matched the expected trajectory.
Bottom Line for Clinical Practice
Neutralizing anti–IL-10 autoantibodies are present in 3.5% of IBD patients and zero healthy controls - this is a biologically specific, not incidental, finding.
Anti–IL-10 seropositivity is strongly associated with HLA-DRB1*01:03 carriage (OR 25–50 across cohorts). In a refractory IBD patient, positive HLA-DRB1*01:03 genotyping substantially raises the pre-test probability for this subtype and warrants anti–IL-10 antibody testing.
This subgroup spans both Crohn's disease and ulcerative colitis - the phenotypic classification tells you nothing about mechanism.
The therapeutic implication is mechanistically distinct from standard IBD biologics: B-cell depletion to reduce autoantibody titer, not downstream cytokine blockade. One published case achieved conventional therapy withdrawal after B-cell depletion.
Testing is not yet standard of care, but HLA-DRB1*01:03 genotyping and anti–IL-10 autoantibody assays are available at specialist centers. Refractory cases - especially those with unexplained biologic non-response - should prompt escalation of immunological workup, not just escalation of biologic therapy.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.