02/05/2026
4viewsAspirin After Colon Cancer Surgery: Who Actually Benefits in 2026?
Aspirin after colon cancer surgery may cut recurrence by 40% in patients with PI3K/PTEN pathway mutations — here's the evidence and who qualifies.
Quick Answer
Aspirin after colon cancer surgery may cut recurrence by 40% in patients with PI3K/PTEN pathway mutations — here's the evidence and who qualifies.
Your patient has just completed resection for stage III colon cancer. Chemotherapy is finished. The oncology team has signed off. And someone in the room asks: "Should we start aspirin?" It's a deceptively simple question with a nuanced, mutation-specific answer - and getting it wrong in either direction has real consequences. This post walks through exactly what the evidence says and the molecular subgroup where aspirin's postoperative benefit is now difficult to ignore.
The challenge with aspirin in colorectal cancer is not a lack of data - it's a lack of precision. Decades of observational studies show population-level benefits. But routine use in all CRC patients post-surgery isn't supported, and for good reason: the benefit is not evenly distributed. What has crystallised from recent prospective data is that aspirin after colon cancer surgery in patients with PI3K/PTEN pathway mutations represents a pharmacologically coherent, increasingly evidence-backed adjuvant strategy. Approximately 37% of all CRC patients carry these alterations. That is not a niche subgroup. Understanding the mechanism - and the trials - is now part of the informed gastroenterologist's toolkit.
How Aspirin Acts on the Colorectal Tumour Microenvironment
Aspirin's oncological effects operate through three distinct biological compartments, each relevant to colorectal carcinogenesis.
At the platelet level, aspirin irreversibly inhibits COX-1, reducing thromboxane A2 production and platelet aggregation. Beyond haemostasis, this limits tumour cell adhesion to the vascular endothelium - a critical early step in haematogenous metastasis.
In inflammatory and immune cells, aspirin downregulates COX-2-derived prostaglandin E2 (PGE2). PGE2 is not a bystander in CRC biology; it actively suppresses anti-tumour immune responses, promoting the immune evasion that characterises advanced colorectal disease. Reducing PGE2 effectively loosens that immune tolerance.
The most mechanistically compelling compartment for postoperative use is the colonocyte itself. Reduced PGE2 directly modulates proliferative signalling through pathways including PI3K, PTEN, APC, RAS, and MAPK. In tumours where PI3K or PTEN is already altered, this PGE2 suppression hits a particularly vulnerable node. Aspirin also acts through PGE2-independent pathways: inhibition of NF-κB and induction of cytochrome C release from mitochondria, both of which tilt the cellular balance toward apoptosis.
This mechanistic specificity - aspirin acting most powerfully where PI3K/PTEN signalling is already dysregulated - is precisely why tumour molecular profiling is not optional when considering adjuvant aspirin. It is the entry criterion.
Per data presented at the Francophone Days of Hepatology, Gastroenterology, and Digestive Oncology 2026 (Paris), the combined PI3K/PTEN alteration cohort now has prospective survival data to accompany this mechanistic rationale.
Clinical Scenario
A 59-year-old woman undergoes right hemicolectomy for a T3N1 sigmoid adenocarcinoma. She completes six months of FOLFOX without significant toxicity. Tumour molecular profiling - obtained at diagnosis as part of standard workup - shows a PIK3CA exon 9 mutation and PTEN loss by immunohistochemistry. She has no history of peptic ulcer disease and takes a low-dose statin for dyslipidaemia.
At her three-month post-chemotherapy review, the question of aspirin is raised. Given her confirmed PI3K/PTEN alteration, the evidence supports initiating low-dose aspirin at 100–160 mg daily. The conversation documents the rationale, acknowledges that large-scale randomised confirmation is still awaited, and establishes a review point at 12 months. She is counselled on GI bleeding risk and given a clear threshold for stopping. The decision is made jointly, documented explicitly, and not made by default.
he Postoperative Trial Data: What We Actually Know
The hypothesis that PI3K-mutated tumours are selectively sensitive to aspirin was first raised in a 2012 publication reporting an HR of 0.18 for CRC recurrence in PI3K-mutant patients taking postoperative aspirin - a striking signal that generated immediate interest in prospective validation.
Two trials have since moved the evidence forward.
A Swiss prospective study randomised 112 patients with PI3K mutations to aspirin 100 mg daily for three years post-surgery. Four-year disease-free survival improved (HR 0.57), though the result did not reach statistical significance - a limitation attributable in part to sample size.
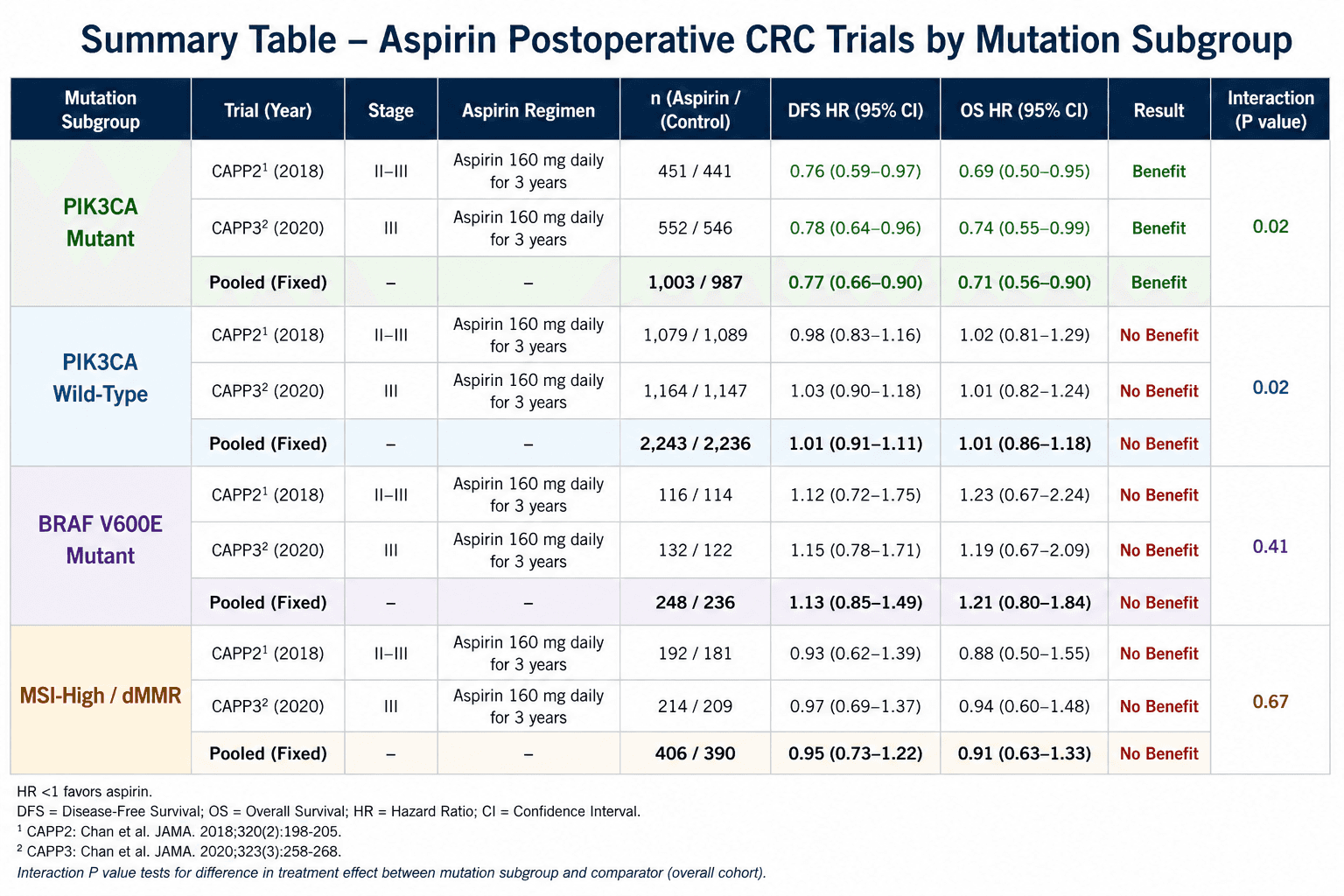
A larger Swedish study enrolled nearly 3,000 patients with PI3K alterations, with 515 receiving aspirin 160 mg daily for three years. Three-year disease-free survival again improved (HR 0.61; 95% CI, 0.34–1.08) without crossing the significance threshold. However, when the analysis was extended to patients with combined PI3K and PTEN pathway abnormalities - 588 patients - aspirin was associated with a statistically significant survival benefit (HR 0.51; 95% CI, 0.29–0.88) and a 40% reduction in recurrence risk (HR 0.42; 95% CI, 0.21–0.83).

A third trial is expected to report in 2026. Until those data land, the current position is this: low-dose aspirin (100–160 mg/day) is a clinically reasonable adjuvant consideration in patients with confirmed PI3K/PTEN pathway alterations, representing roughly 37% of all CRC cases. It is not standard of care - but it is no longer a fringe hypothesis.
A Frequently Overlooked Point: The Mutation Profile Must Come Before the Prescription
The most common error in this space is not refusing aspirin - it is offering it without verifying the molecular subtype. Aspirin confers no proven postoperative benefit in PI3K/PTEN-intact tumours, and exposing a patient to indefinite antiplatelet therapy without a molecular rationale is not conservative practice; it is imprecise practice. Routine tumour profiling for PIK3CA mutation and PTEN status is already standard in many centres for prognostic and treatment-selection purposes. If it is not in your workflow, it needs to be. When a patient asks whether aspirin will help them after CRC surgery, the correct answer begins with their tumour's molecular report - not with population-level meta-analyses.
Bottom Line for Clinical Practice
Do not offer routine postoperative aspirin to all CRC patients. The evidence does not support this, and the benefit is molecularly specific.
Check for PI3K and PTEN pathway alterations as part of standard tumour molecular profiling - this is the prerequisite for any aspirin discussion post-surgery.
In patients with combined PI3K/PTEN pathway abnormalities, low-dose aspirin (100–160 mg/day) for three years post-surgery is associated with a statistically significant reduction in recurrence risk (~40%) and improved disease-free survival.
Lynch syndrome remains a separate indication: aspirin 600 mg/day for ≥2 years reduced CRC incidence by 37% in CAPP2 data; dose optimisation studies (300–600 mg) are ongoing.
Aspirin is not the primary prevention for the general population. The population-level benefit in observational studies is largely concentrated in individuals with cardiovascular risk factors already on antiplatelet therapy.
If you are managing a CRC patient post-surgery and want to work through the molecular profile, recurrence risk, and adjuvant options - including aspirin - bring the case to GastroAGI. Walk it through the clinical details and get a structured, evidence-anchored response in seconds. It will not replace your judgement. It will sharpen it.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.