15/07/2026
16viewsBSG 2026 Adult Coeliac Disease Guideline: What Gastroenterologists Need to Know
BSG’s 2026 adult coeliac disease guideline clarifies testing, biopsy decisions, gluten challenge, follow-up, DXA and refractory disease care.
Quick Answer
BSG’s 2026 adult coeliac disease guideline clarifies testing, biopsy decisions, gluten challenge, follow-up, DXA and refractory disease care.
Introduction
The British Society of Gastroenterology has released its 2026 guideline on the diagnosis and management of adult coeliac disease, updating standards for a condition that remains common, under-recognised, and clinically heterogeneous. The guideline was developed by a multidisciplinary panel and focuses on evidence-based diagnosis, long-term management, follow-up, nutritional assessment, and refractory coeliac disease care.
For gastroenterologists, this update is important because coeliac disease is no longer just a “positive serology plus duodenal biopsy” diagnosis in every adult. The guideline acknowledges newer evidence around serology-based diagnosis, gluten challenge, follow-up intensity, mucosal healing, bone health, vaccination, and referral pathways for complex disease.
The practical message is not that biopsy has become obsolete. Rather, the guideline moves adult coeliac care toward a more individualised model: test correctly, biopsy when needed, use no-biopsy diagnosis only in selected circumstances, support the gluten-free diet properly, and identify patients who need structured long-term review.
Why this update matters
Coeliac disease affects the small intestine but often presents beyond the gut. Patients may present with diarrhoea, bloating, weight loss, iron deficiency anaemia, osteoporosis, abnormal liver enzymes, infertility, neurological symptoms, or fatigue. Others are diagnosed through risk-based testing.
The BSG guideline notes that coeliac disease is a chronic autoimmune disorder in genetically predisposed individuals, with a reported prevalence of approximately 1%. It also reiterates that a lifelong gluten-free diet remains the only accepted treatment.
The update matters clinically for three reasons.
First, diagnostic pathways are evolving. Adults with strongly positive IgA-tTG may, in selected circumstances, be diagnosed without duodenal biopsy, but this requires careful selection and shared decision-making.
Second, follow-up is being reframed. Rather than assuming every patient needs indefinite routine clinic review, the guideline supports structured follow-up early after diagnosis, then patient-initiated follow-up for stable responders, while reserving systematic long-term follow-up for higher-risk groups.
Third, the guideline gives practical direction for non-responsive and refractory coeliac disease, including when to refer to specialist centres and how to assess suspected refractory coeliac disease.
What the guideline found
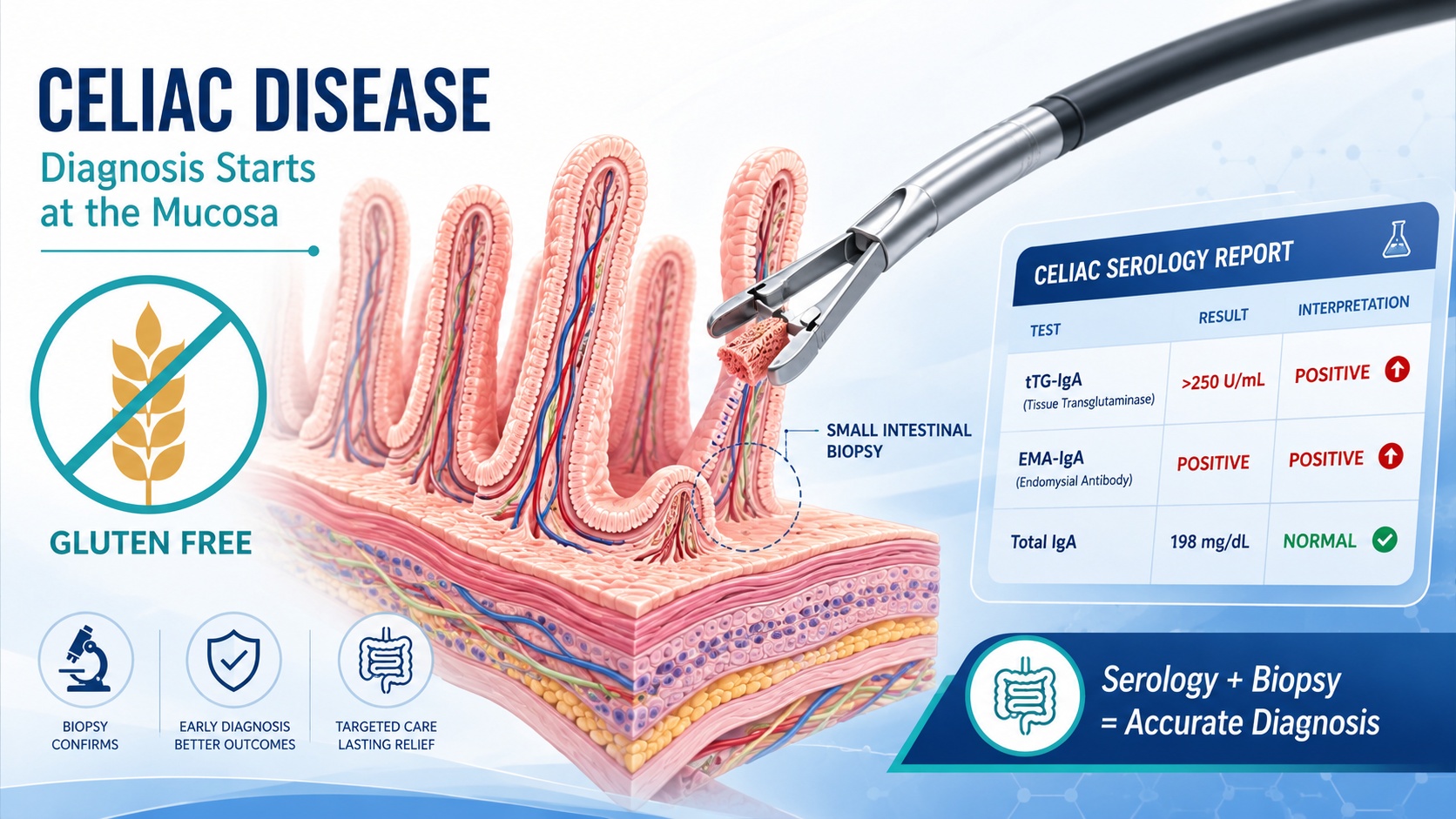
A key diagnostic recommendation is that patients should be consuming a gluten-containing diet before testing. The guideline recommends IgA-tissue transglutaminase antibodies as the first-line investigation and advises screening for selective IgA deficiency alongside IgA-tTG testing.
When biopsy is required, the guideline recommends taking at least four biopsies from the second part of the duodenum and two from the duodenal bulb. This is clinically important because patchy disease and inadequate sampling can lead to missed diagnosis.
One of the most discussed updates is the optional adult no-biopsy pathway. In symptomatic adults assessed in secondary care, the guideline suggests that coeliac disease can be diagnosed without duodenal biopsies when IgA-tTG is at least 10 times the upper limit of normal. However, this is a conditional recommendation, intended for shared decision-making rather than automatic use.
The guideline also cautions against using a lower tTG threshold for a no-biopsy diagnosis because it may increase false-positive diagnoses. It also advises caution in patients with recent autoimmune diagnoses, where false elevation of tTG may be a concern.
For patients already on a gluten-free diet before proper testing, the guideline recommends a gluten challenge of 3–6 g of gluten daily for at least 6 weeks. It notes that duodenal histology is preferred over serology as the diagnostic readout because seroconversion after 6 weeks may be low.
Management continues to centre on a lifelong gluten-free diet. The guideline recommends that patients diagnosed with coeliac disease maintain a lifelong gluten-free diet to improve symptoms, quality of life, and reduce complications. It also recommends a combined approach to assessing gluten-free diet adherence because no single test is adequate alone.
Follow-up is another major practical area. The guideline advises regular follow-up for up to 2 years after diagnosis. After that, patients who respond well may be considered for patient-initiated follow-up, while those with poor adherence, inadequate response, or complications should receive longer-term systematic follow-up.
Nutritional monitoring is emphasised. The guideline advises assessment and monitoring of iron, folate, vitamin B12, vitamin D, and calcium at diagnosis and during follow-up. It also advises DXA scanning 1 year after starting a gluten-free diet in newly diagnosed adults.
For refractory disease, the guideline recommends referral to a specialist centre with an experienced multidisciplinary team. It also recommends flow cytometry to immunophenotype small intestinal intraepithelial lymphocytes as the reference standard for diagnosing refractory coeliac disease type 2.
Clinical interpretation
The most clinically relevant shift is the guideline’s balanced position on the no-biopsy pathway. It does not remove the role of endoscopy. Instead, it defines where biopsy may be avoided and where it remains essential.
This distinction matters. A patient with classic symptoms, high IgA-tTG, appropriate clinical setting, and informed preference may reasonably avoid biopsy under the guideline framework. But patients with equivocal serology, IgA deficiency, iron deficiency anaemia undergoing endoscopy, possible seronegative disease, alarm features, or concern for alternative diagnoses still need careful endoscopic and histological assessment.
The gluten challenge recommendation is also practical. Many patients start a gluten-free diet before seeing a gastroenterologist. Without adequate gluten exposure, both serology and histology may become falsely reassuring. The guideline’s 3–6 g daily for at least 6 weeks gives clinicians a usable framework, while still recognising tolerability issues.
The follow-up model is also realistic. Clinics cannot provide indefinite specialist follow-up for every stable patient, but early follow-up is important for diet education, symptom assessment, nutritional correction, and adherence support. Patient-initiated follow-up may be reasonable for stable responders, but not for patients with persistent symptoms, abnormal labs, poor adherence, persisting villous atrophy, or complications.
Practical implications for gastroenterologists
For daily practice, the guideline supports a few clear changes.
Do not test for coeliac disease after gluten has already been removed unless the limitations are clearly understood. Encourage gluten-containing diet before initial testing where clinically safe.
Use IgA-tTG first line, but remember to assess IgA deficiency. In selective IgA deficiency, IgG-based serology and duodenal biopsy become more important.
When performing endoscopy for suspected coeliac disease, take enough biopsies: four from D2 and two from the bulb. Under-sampling remains a preventable cause of diagnostic uncertainty.
Consider no-biopsy diagnosis only in selected symptomatic adults in secondary care with IgA-tTG ≥10× upper limit of normal, and only after shared decision-making.
For patients already gluten-free, discuss a structured gluten challenge rather than relying on negative tests.
Follow patients actively for the first 2 years after diagnosis, then individualise long-term review.
Assess micronutrients and bone health, and remember that persistent symptoms after a gluten-free diet require a systematic approach rather than simply advising “stricter gluten avoidance.”
Limitations and caution
This is a guideline, not a single new trial. Some recommendations are based on high or moderate certainty evidence, while others are conditional, consensus-based, or expert opinion. The no-biopsy pathway should not be applied casually, and it may not suit patients with atypical features, possible alternative diagnoses, or situations where histology would change management.
The guideline also acknowledges that follow-up decisions may need to be adapted to local healthcare resources. Patient-initiated follow-up is not the same as discharge without safety-netting.
GastroAGI takeaway
The 2026 BSG adult coeliac disease guideline is a clinically useful update for gastroenterologists. Its main message is precision: diagnose on a gluten-containing diet, use IgA-tTG correctly, biopsy properly when needed, reserve no-biopsy diagnosis for carefully selected adults, support the gluten-free diet with structured follow-up, and refer suspected refractory disease early.
For clinicians, this is a practical roadmap for moving adult coeliac disease care from a one-size-fits-all model toward a more accurate, patient-centred, and risk-based approach.
Reference/source
British Society of Gastroenterology guideline page and full guideline PDF.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.