08/05/2026
6viewsDaraxonrasib in Previously Treated RAS-Mutated Pancreatic Cancer: What the NEJM Phase 1/2 Data Actually Means
Daraxonrasib showed a 29% response rate and 15.6-month median OS in previously treated RAS-mutant PDAC - here's what the NEJM data means in practice.
Quick Answer
Daraxonrasib showed a 29% response rate and 15. 6-month median OS in previously treated RAS-mutant PDAC - here's what the NEJM data means in practice.
.png)
A 61-year-old woman with metastatic pancreatic ductal adenocarcinoma has progressed through FOLFIRINOX. Her KRAS mutation is G12D - not G12C, which means sotorasib and adagrasib are off the table. Until recently, your only option was nanoliposomal irinotecan plus 5-FU or enrollment in a clinical trial, with an expected median overall survival of five to seven months. The Phase 1/2 daraxonrasib trial published in the New England Journal of Medicine in May 2026 changes the calculus.
The second-line treatment landscape for pancreatic ductal adenocarcinoma (PDAC) has been defined by futility for decades. Fewer than 10% of patients respond to second-line chemotherapy, and median survival after progression on first-line therapy sits at five to seven months. KRAS inhibitors disrupted this ceiling in lung cancer, but pancreatic cancer posed a harder problem - the mutations are different, they're more heterogeneous, and KRAS drives PDAC in its active, GTP-bound "on" state rather than the inactive state targeted by earlier inhibitors. Daraxonrasib is the first RAS(ON) multi-selective inhibitor to enter clinical trials for PDAC, and the results out of this first-in-human trial represent the most credible survival signal this disease has seen in a very long time.
Why Conventional KRAS Inhibitors Don't Work in PDAC - and How Daraxonrasib Is Different
The oncology world celebrated sotorasib and adagrasib as breakthroughs in KRAS G12C-mutant lung cancer, but their application to pancreatic cancer was always going to be limited. KRAS G12C is relatively rare in PDAC - the dominant mutations are G12D, G12V, and G12R, none of which are addressed by those covalent inhibitors. More fundamentally, those agents work by locking KRAS in its inactive GDP-bound state. In PDAC, RAS proteins spend most of their time in the GTP-bound "on" state, actively driving tumor growth, which means the standard inhibitor mechanism has minimal traction.
Daraxonrasib functions as a molecular glue: in combination with cyclophilin A, it blocks the signaling of RAS proteins in their active state. It is multi-selective - capable of targeting multiple RAS variants, including G12D, G12V, and G12R - which matters enormously in a disease where mutation heterogeneity has historically made targeted therapy nearly impossible. More than 90% of pancreatic adenocarcinomas are driven by RAS mutations, meaning the theoretical addressable population for this mechanism is the entire PDAC population, not a small molecular subtype. This is a fundamentally different paradigm than KRAS G12C inhibition, and the clinical data suggest it works.
What the Phase 1/2 Trial Actually Showed
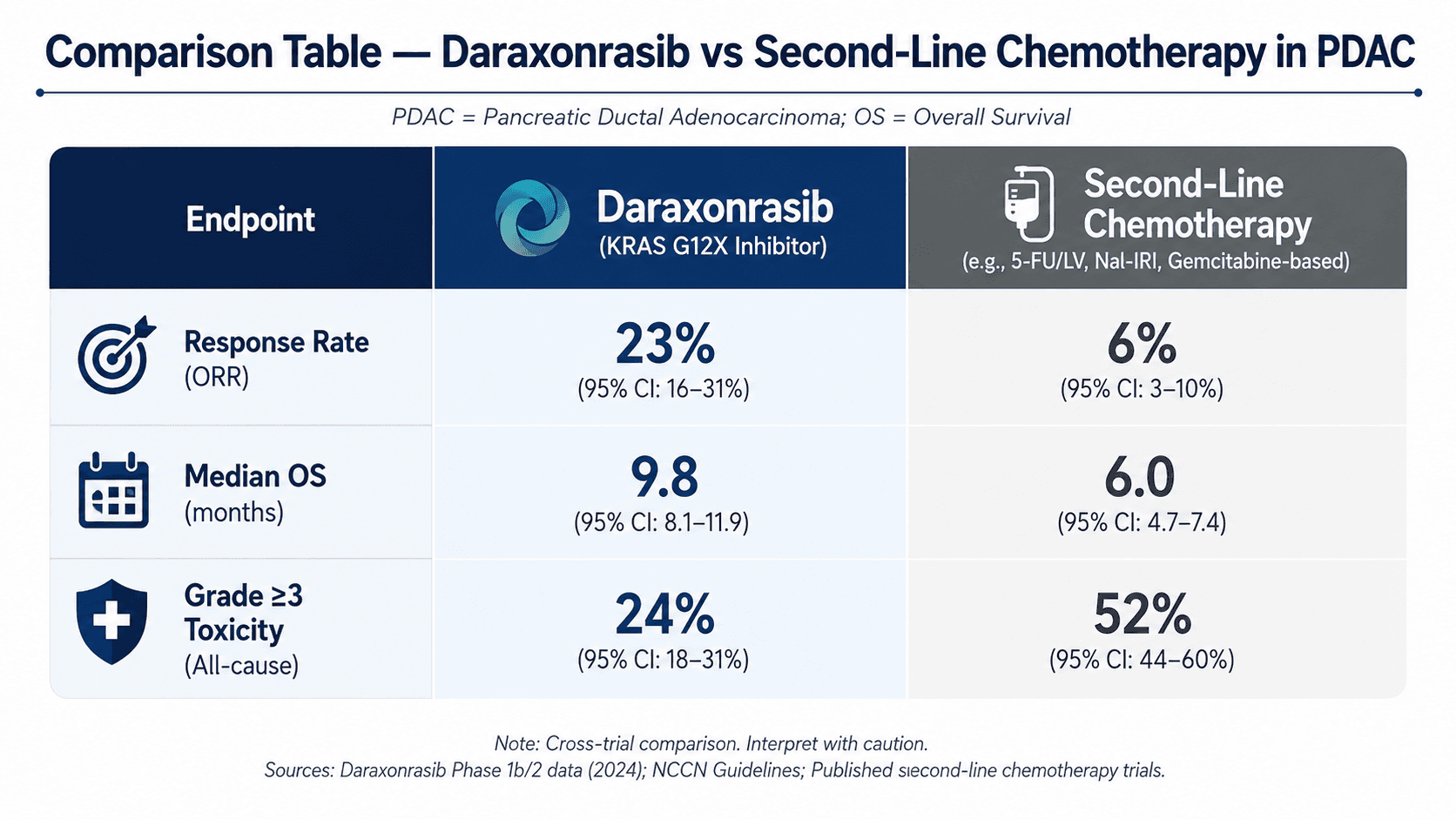
The trial, led by David Hong at MD Anderson and Brian Wolpin at Dana-Farber, was a dose escalation and expansion study with safety as the primary endpoint. Among 38 patients who received the 300 mg dose, the objective response rate was 29% and median overall survival was 15.6 months - roughly three times the historical benchmark for second-line therapy in this population.
The primary endpoint was safety. While 96% of patients experienced adverse effects of any grade, only 30% had grade 3 or higher events. The most common toxicities were rash, diarrhea, stomatitis, mucositis, and fatigue. Half of patients required dose modifications, but no patients discontinued treatment due to adverse effects.
For a disease where second-line cytotoxic regimens like nanoliposomal irinotecan/5-FU carry their own significant toxicity burden, a manageable profile at a therapeutically active dose is a meaningful clinical finding - not just a reassuring footnote. These data were compelling enough that the FDA granted orphan drug designation to daraxonrasib and cleared the path for the ongoing Phase 3 RASolute 302 trial, which is randomising patients to daraxonrasib versus investigator's choice of second-line chemotherapy.
Clinical Scenario: A Patient Who Would Have Had No Good Options
Paragraph 1: A 58-year-old man with stage IV pancreatic ductal adenocarcinoma progressed after six months on modified FOLFIRINOX. Molecular profiling confirmed KRAS G12D mutation. Performance status was ECOG 1. His oncologist had discussed gemcitabine/nab-paclitaxel as a second-line option but noted that expected median survival remained under eight months, and the patient was already experiencing peripheral neuropathy from prior oxaliplatin.
Paragraph 2: Under the RASolute 302 trial eligibility criteria, this patient would be an ideal candidate: measurable disease, ECOG 0–1, RAS G12 mutation confirmed, prior systemic therapy complete. The 29% response rate seen in the Phase 1/2 cohort at 300 mg daily means nearly one in three patients like him would have had a measurable tumour response - with durable remissions reported among responders. His G12D mutation, previously untargetable, was directly addressed by daraxonrasib's multi-selective RAS(ON) mechanism. This is what broad-spectrum RAS inhibition looks like in practice.
Situating This Within the Second-Line PDAC Treatment Decision
Until RASolute 302 reports its primary endpoints, daraxonrasib is not yet standard of care. What clinicians need to understand is how this changes patient conversations right now. For patients with previously treated RAS-mutated PDAC who have maintained adequate performance status, clinical trial enrollment - specifically RASolute 302 - should be an active part of the discussion, not a last resort. The Phase 3 trial enrolled patients with ECOG 0–1, measurable disease per RECIST 1.1, and adequate organ function.
The key practical distinction is mutation profiling. Daraxonrasib can target multiple RAS variants, not just G12C, which means molecular testing is no longer just a prognostic exercise in PDAC - it is a therapeutic prerequisite. Reflex somatic profiling at the time of diagnosis now has direct implications for second-line eligibility. If a patient progresses on first-line therapy without documented mutation status, the window for relevant second-line intervention may be narrowed unnecessarily.
For community gastroenterologists and GI oncologists managing PDAC, the immediate action is to ensure molecular profiling is ordered at diagnosis, not after progression. The infrastructure for targeted therapy is being built now, and patients who arrive to second-line decisions without a molecular profile miss a rapidly closing opportunity.
A Frequently Overlooked Point: RAS "Wild-Type" Patients Were Also Enrolled
The RASolute 302 Phase 3 trial includes patients without an identified RAS mutation - so-called wild-type PDAC. This is worth noting because "RAS wild-type" at standard clinical sequencing does not guarantee truly RAS-independent biology; low-allele-fraction mutations and technical assay limitations are real confounders. More importantly, the trial's inclusion of wild-type patients means the signal from RASolute 302 will inform treatment decisions across the full PDAC population, not just the 90% with confirmed mutations. Clinicians should not automatically exclude a patient from referral to trial on the basis of wild-type status pending the trial's full reporting.
Bottom Line for Clinical Practice
Order reflex somatic molecular profiling at PDAC diagnosis, not at progression - RAS mutation subtype (G12D, G12V, G12R) now directly determines second-line trial eligibility.
For patients progressing after first-line chemotherapy with ECOG 0–1, discuss RASolute 302 enrollment alongside standard second-line options; the Phase 1/2 data show a 29% ORR and 15.6-month median OS at 300 mg daraxonrasib.
Do not conflate KRAS G12C inhibitors (sotorasib, adagrasib) with daraxonrasib - the mechanism is fundamentally different; daraxonrasib targets RAS in its active GTP-bound state and covers the mutations that actually predominate in PDAC.
Grade ≥3 toxicity was seen in 30% of patients - rash, diarrhea, and stomatitis are the signals to watch; no patients discontinued due to toxicity, but proactive monitoring and dose modification protocols matter.
RASolute 302 is enrolling now - this is the moment to identify eligible patients early rather than at end-stage disease when performance status excludes trial participation.
When you're managing a patient with progressive RAS-mutated PDAC and weighing second-line options, bring the clinical details to GastroAGI - it will walk through eligibility considerations, mutation-specific therapy options, and guideline-aligned management in real time. The landscape is shifting faster than any single update can capture.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.