11/05/2026
15viewsDDW 2026 Highlights: Day-by-Day Conference Insights for Gastroenterologists
DDW 2026 in Chicago covered EUS, pancreatitis, IBD, bariatric endoscopy, CRC screening, and more. Day-by-day clinical takeaways for GI practitioners
Quick Answer
DDW 2026 in Chicago covered EUS, pancreatitis, IBD, bariatric endoscopy, CRC screening, and more. Day-by-day clinical takeaways for GI practitioners
You couldn't be everywhere at DDW 2026. Four days, hundreds of sessions, thousands of attendees across McCormick Place - and the signal-to-noise ratio was unforgiving. This post cuts straight to what mattered: the clinical themes that surfaced repeatedly, the practice-changing debates, and the takeaways that will follow you into clinic long after the Chicago wind fades. Day by day.
What DDW 2026 Was Really About
Digestive Disease Week 2026 (May 2–5, Chicago) arrived at an inflection point for the specialty. EUS has graduated from a diagnostic tool to a full therapeutic platform. Endoscopy is being reimagined as a surgical discipline. Gut-brain interaction disorders finally got the mechanistic attention they deserved. And for the first time, artificial intelligence wasn't a background conversation - it was embedded in imaging, diagnostics, and clinical decision-making across almost every sub-track.
The DDW 2026 gastroenterology agenda reflected a field in genuine transition. The dominant clinical questions were no longer "can we do this endoscopically?" - that debate is largely settled. The harder questions now are: when should we, how do we train for it, and what does value-based care look like when a GI suite can now do what once required an OR?
Here is how it unfolded.
Day 1 (May 2): Pancreatitis, Pancreatic Cysts, and EUS as the New Standard
The Anchor Topic: Acute Pancreatitis in 2026
Day 1 opened with a strong focus on acute pancreatitis modern management — and the message was clear: the 2024–2025 guideline updates are still not being fully implemented at the bedside. DDW 2026 re-emphasized that fluid resuscitation strategy (Lactated Ringer's over normal saline), early oral feeding in mild disease, and avoidance of prophylactic antibiotics remain systematically underutilized. Severity prediction — still the crux of the first 48 hours — was presented through emerging AI-assisted scoring models that integrate SIRS criteria, BUN trajectory, and hematocrit trends more dynamically than static scoring tools like BISAP or Ranson's.
Necrotizing pancreatitis management continued to draw debate. The "step-up" approach remains standard, but Day 1 sessions highlighted how EUS-guided drainage of walled-off necrosis is consolidating as the preferred first intervention over percutaneous routes at centers with the expertise — with lower rates of pancreatic fistula formation and shorter hospital stays.
Pancreatic Cysts: Rethinking Both Detection and Surveillance
Two separate sessions tackled pancreatic cyst management from complementary angles. The first examined surveillance strategy - specifically, the clinical problem of the vast majority of detected cysts (the majority of which are incidentalomas on cross-sectional imaging) never progressing, yet consuming enormous surveillance resources. The emerging consensus leans toward risk-stratified, time-limited surveillance with clear exit criteria, rather than indefinite annual MRI.
The second session pushed beyond fluid analysis: multimodal EUS assessment using AI-enhanced imaging, through-the-needle biopsy, and cyst fluid proteomics is improving discrimination between mucinous and non-mucinous lesions. The clinical takeaway - fluid CEA alone is insufficient. A high-risk mucinous cyst with low CEA is not a low-risk cyst.
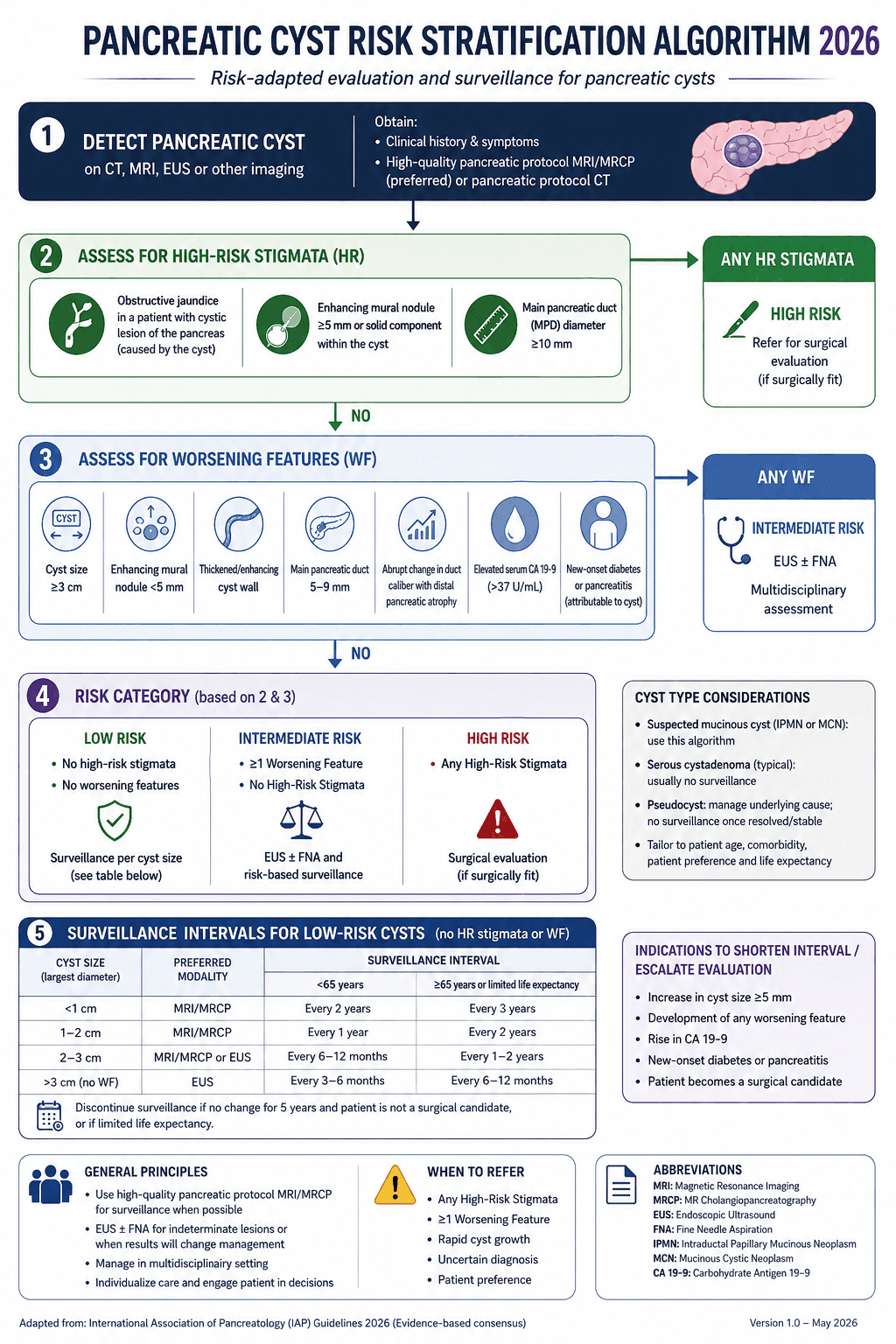
Clinical Scenario
A 67-year-old woman with a 3.2 cm branch-duct IPMN detected incidentally on CT for renal colic. No worrisome features on initial MRI. CEA in cyst fluid: 38 ng/mL. She has been on annual MRI surveillance for four years, with stable morphology.
At DDW 2026 sessions, this case was presented as exactly the type where newer multimodal EUS - incorporating confocal laser endomicroscopy and next-generation cyst fluid molecular markers - could support a shared decision to exit surveillance in a low-risk profile, rather than committing to indefinite follow-up with its costs, patient anxiety, and incidental findings. The question being asked at DDW is no longer "do we watch this?" but "how long, with what, and when do we stop?"
Day 2 (May 3): EUS Expands, IBD Gets Structural, Endoscopy Meets Surgery
EUS: From Diagnosis to Therapeutic Platform
Day 2 consolidated EUS's place as one of the fastest-evolving areas in gastroenterology. Four distinct themes ran through EUS-focused sessions:
EUS-guided biliary drainage (EUS-BD) was presented as a genuine first-line alternative to ERCP in select patients - not merely a rescue strategy for failed cannulation. The evidence base supporting EUS-hepaticogastrostomy and EUS-choledochoduodenostomy has matured enough that several centers are now offering EUS-BD as primary drainage in distal malignant obstruction with favorable anatomy. DDW 2026 sessions stressed that this shift requires operator volume, structured training, and outcome benchmarking - the technique is not interchangeable with ERCP in the hands of the occasional user.
EUS in chronic pancreatitis was reframed as a therapeutic decision-support tool - not just for parenchymal/ductal assessment, but for guiding celiac plexus interventions and staging severity in ways that influence whether a patient is routed to ERCP, surgery, or pain-focused medical management.
Interventional EUS in the lower GI tract - EUS-guided drainage of pelvic collections, perirectal abscesses, and anastomotic leaks - was positioned as an expanding clinical service with meaningful implications for post-surgical GI care.
EUS as a high-value service was addressed specifically in an economics-focused session: as EUS procedure volumes grow and payer scrutiny intensifies, demonstrating diagnostic yield, procedure pairing efficiency, and downstream decision impact is no longer optional for program sustainability.
Crohn's Strictures: Bowel Preservation as the Explicit Goal
IBD surgery at DDW 2026 centered on Crohn's disease stricture management, with an unmistakable thematic shift: bowel-preserving therapy is now the stated goal, not simply a preference. Endoscopic balloon dilation, EUS-guided stricturoplasty, and biodegradable stenting were all presented with updated outcome data. The DDW 2026 consensus framing was that surgery should follow a failed endoscopic attempt, not precede it, for most short fibrotic strictures. Multidisciplinary decision-making - gastroenterologist, colorectal surgeon, and radiologist - was emphasized as the standard of care, not the exception.
Day 3 (May 4): Esophageal Disorders, Motility, Obesity, and the Gut-Brain Axis
Esophageal Disease: From POEM Complications to Barrett's
Day 3 opened with a clinically rich esophageal surgery session. Recurrent dysphagia after POEM was examined with nuance - distinguishing incomplete myotomy from reflux-related stricture from functional post-procedural dysmotility. The diagnostic reassessment algorithm presented included timed barium swallow, high-resolution manometry re-evaluation, and pH-impedance testing on and off PPI before any re-intervention decision.
Post-EMR bleeding risk stratification received a dedicated session, with updated scoring tools that integrate lesion size, morphology, location, and patient anticoagulation status to stratify risk more precisely than older approaches. DDW 2026 data suggested prophylactic clipping strategy should be tailored to risk category rather than applied uniformly.
Deep mural injury versus true perforation after esophageal dilation was presented as a consistently mismanaged clinical scenario — the instinct to escalate to surgery for a large air collection without clinical deterioration is often wrong, and updated management algorithms favor conservative endoscopic closure with NPO and IV antibiotics for selected transmural injuries.
Barrett's esophagus with low-grade dysplasia was given a focused session: surveillance intervals, endoscopic eradication therapy (EET) timing, and the emerging data supporting earlier EET in confirmed LGD on expert pathology review.
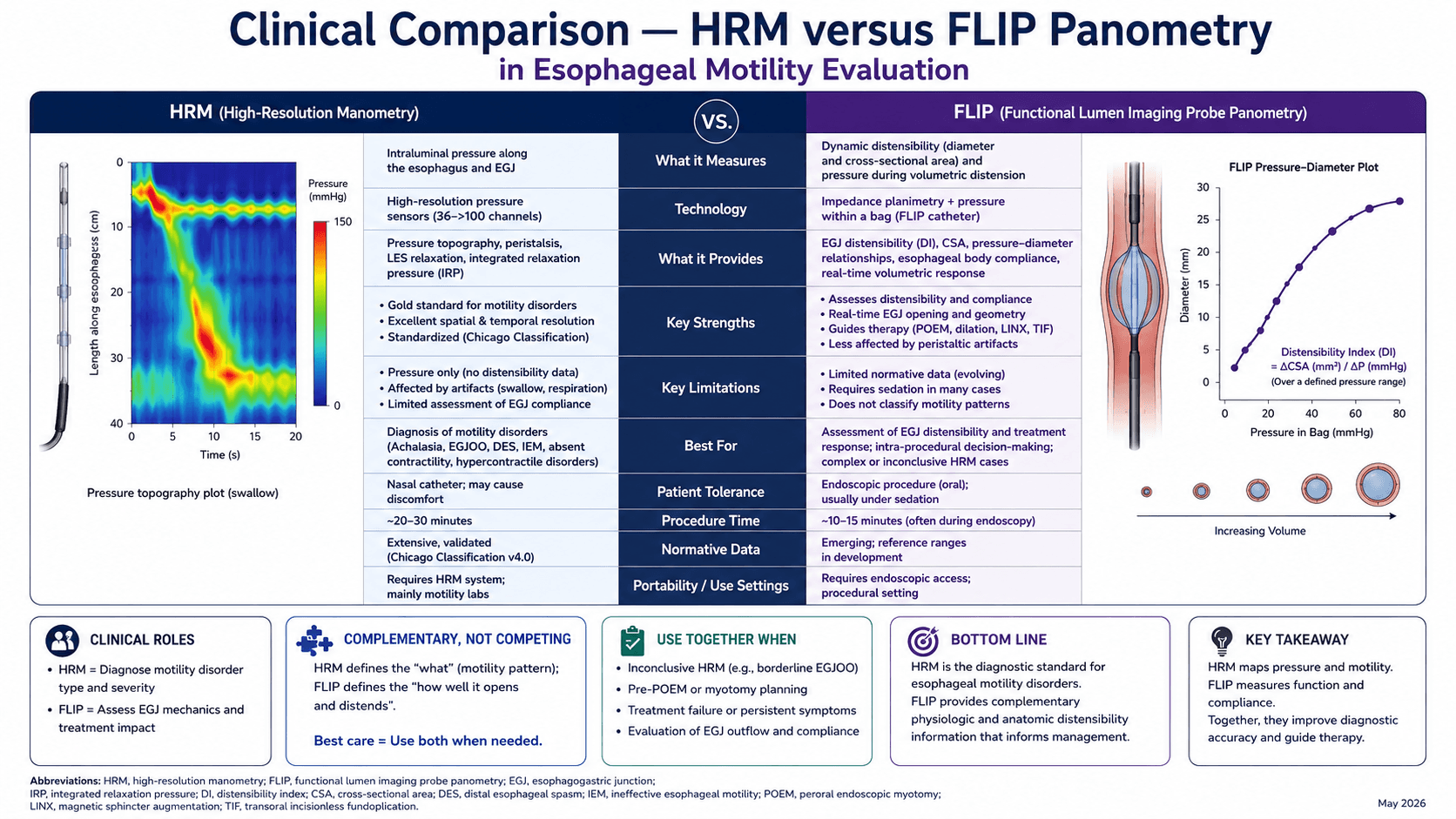
Motility: FLIP Panometry Changes the Conversation
Translational physiomechanics and FLIP panometry was one of the more intellectually dense Day 3 sessions. The key clinical message: conventional high-resolution manometry frequently fails to explain patient symptoms in functional dysphagia and non-obstructive dysphagia. FLIP panometry - measuring distensibility and contractile response - identifies clinically significant esophagogastric junction dysfunction that HRM misses. DDW 2026 presenters argued that FLIP should move from a supplementary to an integrated first-line tool in esophageal motility evaluation, particularly in post-fundoplication or post-POEM symptom recurrence.
Obesity and Metabolic Endoscopy: A Specialty of Its Own
The metabolic track at DDW 2026 was arguably the highest-energy programming of the conference.
Metabolic surgery was presented through a long-term outcomes lens: 10+ year data from RYGB and sleeve gastrectomy cohorts confirmed durable T2DM remission and cardiovascular risk reduction, but also highlighted the significant subset with weight recurrence and metabolic relapse requiring reintervention. The integrated care model - bariatric surgery plus GLP-1 receptor agonist therapy plus psychological support was presented as the new standard.
Endoscopic bariatric therapy (EBT), and specifically endoscopic sleeve gastroplasty (ESG) - received major airtime. ESG is now the most widely performed EBT procedure globally, and DDW 2026 data presented weight loss outcomes at 18-24 months that are competitive with sleeve gastrectomy in appropriately selected patients. The discussion shifted from "does ESG work?" to "who is the optimal ESG candidate, and how do we integrate it with pharmacotherapy?" Metabolic endoscopy as a subspecialty designation - distinct from bariatric surgery is a DDW 2026 conversation that will have structural implications for GI training programs.
Gut-Brain Axis: Finally Getting the Mechanistic Attention It Deserves
Functional dyspepsia and gastroduodenal disorders were presented in two separate sessions - one focused on evolving gut-brain and immune paradigms, one on overlapping clinical presentations. The mechanistic picture now includes duodenal eosinophilia, mast cell activation, impaired mucosal barrier function, and altered central pain processing - none of which are captured in Rome IV criteria. DDW 2026 signaled that the diagnostic and treatment approach to functional dyspepsia is about to change substantially as these mechanisms become treatable targets.
Nutritional interventions in DGBI - covering diet, microbiome, and gut-brain interaction - were presented with updated evidence on low-FODMAP diet implementation, specific carbohydrate diet, and probiotic stratification. POTS, hEDS, and gut dysmotility emerged as an increasingly recognized clinical cluster, with DDW 2026 sessions flagging that GI symptoms in these patients are frequently misattributed to functional disorders, delaying appropriate connective tissue-oriented workup.
Day 4 (May 5): Screening, Training, Economics, and the Future of Endoscopy
CRC Screening: Expanding Access Without Losing Precision
The colorectal cancer screening track on Day 4 tackled a genuinely complex landscape.
Stool-based testing integration - specifically FIT and multi-target stool DNA - was examined in the context of screening uptake gaps. Despite strong guideline endorsement, CRC screening rates remain suboptimal in low-resource and underserved settings. DDW 2026 presented primary care-GI integration models and patient navigation strategies that meaningfully improve uptake. The clinical message: the best screening test is the one the patient will actually do.
Blood-based CRC screening (cell-free DNA and methylation-based assays) received a dedicated session examining where these tests fit in the clinical pathway. Sensitivity for CRC is strong; sensitivity for advanced adenoma remains the limiting factor. DDW 2026 framing: blood-based tests expand access and are appropriate for screening-reluctant patients, but positive results require colonoscopic confirmation and negative results do not replace colonoscopy for high-risk individuals.
CRC in India was addressed in a separate global health session - highlighting distinct epidemiological features, delayed presentation, limited surgical infrastructure, and the opportunity for endoscopy-led early detection strategies in a rapidly urbanizing, high-risk demographic.
Endoscopy Education: Competency-Based Training is Now the Standard
Two full sessions addressed the transformation of endoscopy training, and both sent the same message: the apprenticeship era is over.
Competency-based medical education (CBME) in endoscopy - using simulation, structured feedback, EHR-integrated quality metrics, and direct observation tools - was presented as the new training architecture. The fellow's perspective session was particularly pointed: current trainees are graduating into practice environments with volume-based expectations that competency-based training programs have not yet fully aligned with.
Mastering endoscopy education focused on how high-volume, high-complexity programs (ESD, EUS, POEM, ESG) require purpose-built curricula that traditional case-number milestones cannot capture. DDW 2026's message to training program directors: redesign around skill acquisition curves, not case counts.
Economics and Service Line Design
The closing economics track was one of the more practical DDW 2026 contributions for program leadership. Expanding gastroenterology service lines in an era of declining procedural reimbursement, healthcare consolidation, and payer scrutiny requires GI practices to demonstrate clinical value - not just volume. Panelists presented models for quality dashboard integration, downstream referral capture, and EHR-anchored outcomes reporting as tools for payer contract negotiation. The colonoscopy quality dashboard session specifically showed how EHR analytics can drive system-level improvement in adenoma detection rates, withdrawal times, and bowel prep quality across a multi-site practice.
The Four Overarching Themes of DDW 2026
Stepping back from the day-by-day: four themes ran through almost everything at DDW 2026.
1. EUS is a therapeutic subspecialty now. Biliary drainage, pancreatic cyst ablation, lower GI interventions, chronic pancreatitis management - EUS is not an add-on to endoscopy. Programs without structured EUS training pipelines are already behind.
2. Gut-brain interaction is mechanistically tractable. Functional dyspepsia, IBS, DGBI overlapping disorders, POTS/hEDS - the days of "nothing structural, reassure the patient" are ending. The pathophysiology is being defined, and treatable mechanisms are being identified.
3. AI is embedded, not emerging. AI-integrated EUS imaging, colonoscopy quality analytics, pancreatic cyst characterization, and CRC screening pathway optimization were not featured as "future" tools. They were presented as current clinical applications being implemented now.
4. Training must catch up to the procedures. ESG, ESD, POEM, EUS-BD - these are complex interventional skills. DDW 2026 sent an unambiguous message: competency-based training frameworks, simulation curricula, and structured mentorship models are not optional for programs offering these services.
A Frequently Overlooked Point from DDW 2026
The sessions on ERCP in elderly patients with choledocholithiasis - specifically the target trial emulation data re-examining early ERCP - deserve attention beyond the conference. The conventional teaching that all common bile duct stones require early ERCP is being challenged by real-world data showing that appropriately selected elderly patients with uncomplicated choledocholithiasis and no cholangitis or pancreatitis can be managed with watchful waiting followed by elective ERCP, without increased adverse events. In a population already carrying high sedation risk, this is clinically important. The reflex to scope within 24 hours in every elderly patient with a stone should be reconsidered.
Stay Current Without the Conference
DDW runs for four days. The literature that follows it runs for four years. GastroAGI tracks emerging evidence across pancreatology, advanced endoscopy, IBD, hepatology, and motility disorders - and brings it into real clinical questions. Walk GastroAGI through a post-DDW clinical scenario: the next complex EUS case, the pancreatic cyst you're not sure whether to keep watching, the functional dyspepsia patient who has failed two PPI trials. You'll get a reasoned, guideline-anchored response built from the same evidence base that drove the conversations in Chicago.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.