21/04/2026
8viewsGut Microbiome Research in India: What the Evidence Shows, What It Doesn't, and What to Do With It Clinically
What Indian microbiome research has revealed clinically, where the evidence gaps remain, and what gastroenterologists should do with it now.
Quick Answer
What Indian microbiome research has revealed clinically, where the evidence gaps remain, and what gastroenterologists should do with it now.
.png)
A 34-year-old vegetarian woman from Chennai presents with bloating, loose stools, and abdominal cramps for two years. Her colonoscopy is normal. Her H. pylori test is negative. You diagnose IBS-D - but you're treating her with protocols built almost entirely on Western microbiome data, in a patient whose gut flora has almost nothing in common with the cohorts those studies used. That gap is no longer just academic. This post maps what gut microbiome research in India has actually shown, where the critical unknowns remain, and how to use the emerging data in clinical practice today.
The gut microbiome research field accelerated globally after 2012, but the dominant datasets - HMP (Human Microbiome Project), MetaHIT, UK Biobank - were built almost entirely on Western, industrialised populations. Indian patients eat differently, carry different early-life exposures, have higher rates of H. pylori colonisation, lower rates of red meat consumption, and distinct patterns of antibiotic use. The downstream effect on the gut microbiota is substantial. Gut microbiome research in India has now produced enough data to challenge several assumptions clinicians make daily: about what "normal" flora looks like in Indian adults, which microbial signatures associate with IBS, NAFLD, and colorectal cancer in this population, and whether probiotic or dietary recommendations from Western RCTs translate meaningfully to Indian patients. The honest answer to most of those questions is still "incompletely." But the outlines are getting clearer.
What the Indian Microbiome Actually Looks Like - And Why It Matters Clinically
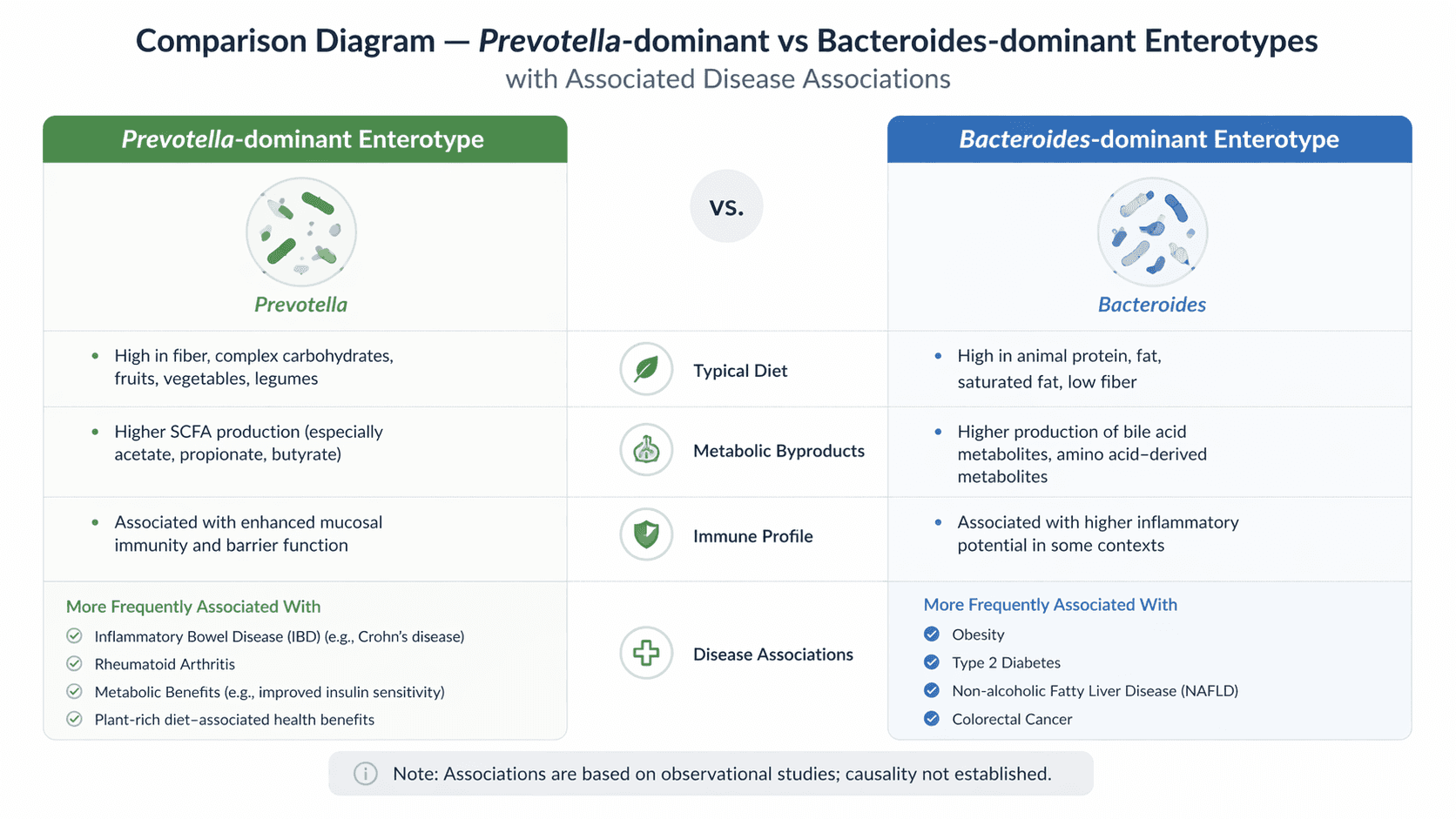
The landmark 2020 study from the Indian Genome and Microbiome Initiative characterised the gut microbiota of over 1,000 healthy Indian adults across multiple geographic and dietary strata. The findings departed meaningfully from Western reference ranges. Prevotella-dominant enterotypes - rare in European cohorts - were the predominant pattern in rural and semi-urban Indian adults, particularly among those on plant-rich, low-meat diets. Bacteroides-dominant profiles, which underpin most Western dysbiosis research, were less common and skewed toward urban, Westernised dietary patterns.
This is not a trivial distinction. Most probiotic studies, and most mechanistic dysbiosis research linking specific taxa to disease, were conducted in Bacteroides-dominant populations. A patient whose baseline flora is Prevotella-dominant responds differently to the same dietary perturbation or antibiotic course - the "return to baseline" trajectory is different, the metabolite outputs (short-chain fatty acids, bile acid profiles) differ, and the inflammatory signalling patterns are not the same. Per a 2023 review in Gut, Prevotella copri - highly prevalent in South Asian cohorts - is now associated with both immune modulation in healthy individuals and proinflammatory signalling in susceptible ones, depending on strain and host context. Treating Indian gut flora as a minor variant of Western gut flora is a clinical approximation that is becoming harder to justify as the data accumulates.
Clinical Scenario
A 48-year-old male farmer from rural Maharashtra is referred for evaluation of recurrent non-bloody diarrhoea, weight loss of 4 kg over six months, and fatigue. Full workup including colonoscopy, duodenal biopsy, and stool culture is negative. CECT abdomen is normal. Coeliac antibodies are negative. His diet is predominantly plant-based - jowar, dal, seasonal vegetables, minimal processed food. He has taken three courses of broad-spectrum antibiotics over the past two years for respiratory infections.
Stool 16S rRNA sequencing (available at a few tertiary centres now) showed severe depletion of Faecalibacterium prausnitzii and Roseburia, with relative overgrowth of Proteobacteria - a pattern consistent with post-antibiotic dysbiosis in a Prevotella-dominant baseline. Management focused on dietary optimisation (high-fermentable fibre to support butyrate-producing taxa), a 4-week course of a well-characterised multi-strain probiotic, and avoidance of further unnecessary antibiotics. Symptoms improved substantially at 3-month follow-up. This case illustrates both the clinical relevance of antibiotic-driven dysbiosis in Indian patients and the limits of managing it without knowing the patient's baseline microbiome architecture.
Where Indian Microbiome Research Has Found Signal -> IBS, NAFLD, and Colorectal Cancer
Three disease areas now have enough India-specific data to inform clinical thinking.
IBS: A 2022 multicentre study across Chennai, Mumbai, and Delhi found that Indian IBS-D patients showed consistent depletion of Lactobacillus and Bifidobacterium species alongside elevated Escherichia and Shigella - broadly consistent with global IBS microbiome literature. However, the magnitude of Prevotella depletion was unique to the Indian cohort and inversely correlated with symptom severity. This suggests Indian IBS patients may have a distinct microbial signature that affects how well they respond to standard probiotic regimens (which typically contain Lactobacillus and Bifidobacterium but not Prevotella-supporting substrates).
NAFLD: The Indian NAFLD microbiome phenotype - studied in cohorts from AIIMS Delhi and Christian Medical College Vellore - shows elevation of Ruminococcus gnavus and Clostridium leptum alongside reduction in Akkermansia muciniphila, consistent with gut barrier dysfunction and metabolic endotoxaemia. The dietary context matters here: high refined carbohydrate intake in urban Indians, combined with a baseline microbiome not adapted to metabolise it efficiently, may accelerate hepatic fat accumulation through a microbiome-mediated pathway. This is not yet practice-changing evidence, but it shifts the clinical conversation about NAFLD management beyond just calories and glycaemic control.
Colorectal cancer:Fusobacterium nucleatum enrichment in tumour tissue - now a recognised CRC microbiome marker globally — has been confirmed in Indian CRC cohorts. A 2024 study from Tata Memorial Centre found Fusobacterium prevalence in Indian CRC tissue comparable to Western data, suggesting this marker may have diagnostic or prognostic relevance regardless of dietary background. Research into whether faecal microbiome signatures could supplement colonoscopic screening in resource-limited Indian settings is ongoing.
A Frequently Overlooked Point: The Antibiotic Exposure Problem in Indian Patients
Indian patients carry one of the world's highest burdens of antibiotic overuse - over-the-counter access, frequent empiric courses, and high rates of childhood antibiotic exposure during diarrhoeal illness all compound. What this means clinically is that a substantial proportion of patients presenting with functional GI symptoms, chronic diarrhoea, or unexplained fatigue have acquired dysbiosis - not from their baseline diet or genetics, but from years of antibiotic perturbation superimposed on a flora that has limited resilience data. Most probiotic RCTs studied populations with lower cumulative antibiotic exposures. When you recommend a probiotic to an Indian patient who has had six antibiotic courses in four years, you are operating in clinical territory that existing trial data does not adequately cover. Taking an antibiotic history with the same rigour as a drug allergy history is not excessive caution - it is good microbiome medicine.
Bottom Line for Clinical Practice
Treat published Western dysbiosis profiles as a starting reference, not a direct template - the Indian gut microbiome has a distinct baseline that affects how disease signatures and interventions map onto your patients.
In IBS-D, NAFLD, and CRC, India-specific microbiome data now exists and is worth reviewing before making management decisions driven purely by global guidelines.
Take a detailed antibiotic history in all patients with functional GI symptoms - cumulative exposure is a major driver of dysbiosis in the Indian population that often goes undocumented.
Stool microbiome sequencing is available at select tertiary centres in India; consider referral for patients with refractory functional symptoms, post-antibiotic diarrhoea not responding to standard management, or atypical IBS presentations.
Dietary advice should be microbiome-informed - high-diversity plant fibre, fermented foods (curd, kanji, idli), and reduced ultra-processed carbohydrate support a Prevotella-dominant flora better than generic "eat more fibre" instructions.
The evidence is still maturing, but the clinical direction is clear: Indian microbiome data deserves to inform how you manage Indian patients, not just global averages. When you're working through a case where the GI workup is negative but the patient is not well, walk GastroAGI through the details - diet, antibiotic history, geography, symptom pattern - and get a reasoned, evidence-grounded differential that accounts for the full clinical picture.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.