04/05/2026
6viewsHepatic Encephalopathy: West Haven Grading, Identifying the Precipitant, and Step-by-Step Management
Grade HE using West Haven criteria, identify the precipitant driving it, and follow a step-by-step management protocol
Quick Answer
Grade HE using West Haven criteria, identify the precipitant driving it, and follow a step-by-step management protocol
A 58-year-old man with known Child-Pugh B cirrhosis is brought in by his family - he has been sleeping through the day, missing meals, and said something bizarre at dinner last night. His ammonia is elevated, but so is everyone's with decompensated cirrhosis. The real question is not whether this is hepatic encephalopathy - it almost certainly is. The question is what triggered it, what grade it is, and what you do in what order. This post gives you a structured answer to all three.
Hepatic encephalopathy management trips up even experienced clinicians not because the individual steps are difficult, but because the decisions happen in parallel - you are grading, hunting for precipitants, and initiating treatment simultaneously, often in a busy ward or emergency bay. The West Haven Criteria give you the language. The precipitant hunt gives you the lever. The management algorithm gives you the sequence. Miss any one of these, and you are treating a symptom rather than the episode. What makes this harder still is that ammonia levels correlate poorly with grade - a patient can have grade III HE with a modestly elevated ammonia, and a compensated cirrhotic can have a markedly elevated ammonia with minimal clinical findings. The clinical examination, not the lab value, grades the encephalopathy.
West Haven Criteria: Grading Hepatic Encephalopathy at the Bedside
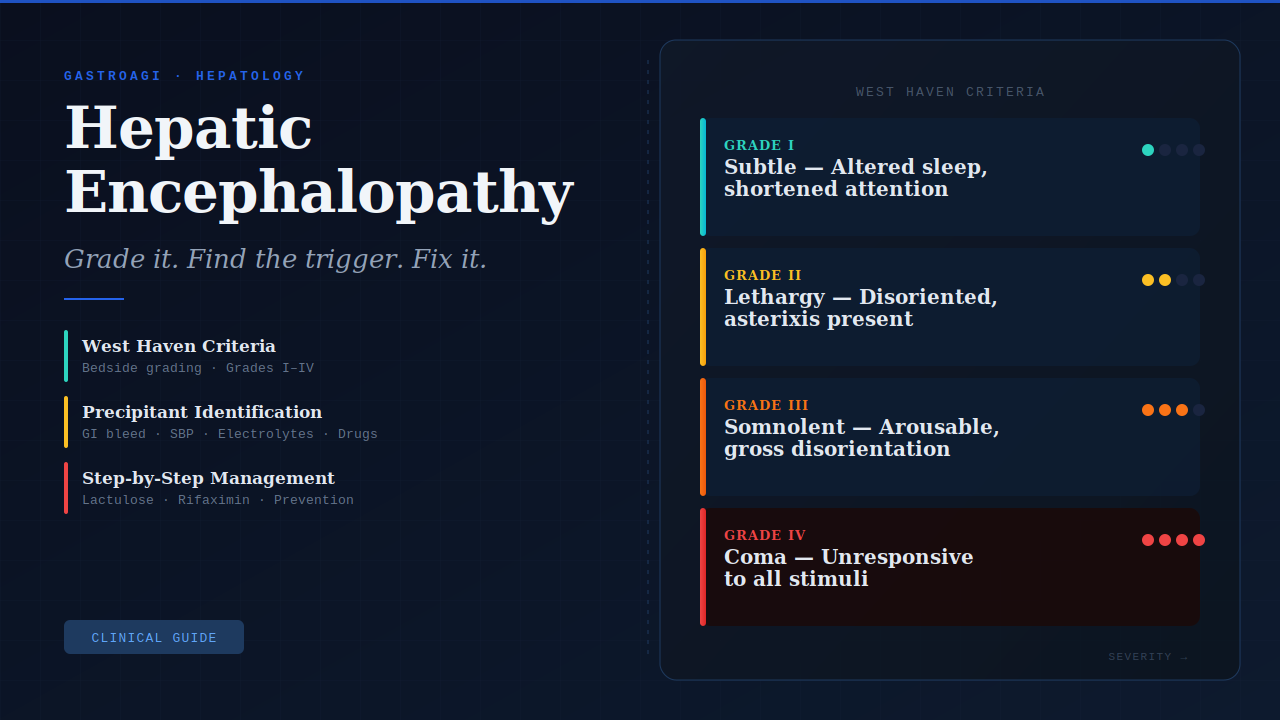
The West Haven Criteria remain the standard grading system endorsed by the International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN) and the AASLD 2014 HE Practice Guidance. Four grades - each with distinct clinical anchors:
Grade I: Trivial lack of awareness, shortened attention span, altered sleep rhythm. The patient is oriented but something is slightly off. Family often picks this up before the clinician does.
Grade II: Lethargy, disorientation to time, obvious personality change, inappropriate behaviour. Asterixis is typically present and detectable. This is the grade where the patient can still hold a conversation but cannot reliably follow commands.
Grade III: Somnolent but arousable. Gross disorientation, bizarre behaviour, asterixis may be difficult to elicit. The patient responds to verbal stimuli but cannot cooperate with examination.
Grade IV: Coma - unresponsive to verbal or painful stimuli. Distinguish decorticate from decerebrate posturing; both indicate grade IV but have different prognostic implications.
Covert hepatic encephalopathy (formerly minimal HE) sits below Grade I - detectable only on psychometric or neurophysiological testing, not at the bedside. It affects up to 80% of cirrhotic patients and is a strong predictor of overt HE within 12 months. The Psychometric Hepatic Encephalopathy Score (PHES) remains the reference standard for covert HE detection, though the EncephalApp Stroop test offers a practical clinical alternative.
One important nuance: grade the patient on their best sustained level of arousal, not their worst moment. Patients fluctuate. The grade that determines management is the ceiling, not the floor.
Clinical Scenario
A 63-year-old woman with hepatitis C-related cirrhosis (Child-Pugh C, MELD 18) presented with two days of worsening confusion. Her husband reported she had been started on a new diuretic dose four days prior for ascites management.
On examination she was somnolent, disoriented to time and place, and had florid asterixis - consistent with West Haven Grade III. Sodium was 128 mEq/L, creatinine had risen to 1.9 mg/dL from a baseline of 0.9, and urine sodium was 8 mEq/L. Ascitic fluid tap revealed a neutrophil count of 380 cells/mm³, confirming spontaneous bacterial peritonitis as a co-existing - and likely primary - precipitant alongside overzealous diuresis.
She was started on cefotaxime for SBP, diuretics were held, gentle IV saline correction was initiated for hyponatraemia, and lactulose was titrated to 3 soft stools per day. Within 48 hours she had improved to Grade I. The lesson: two precipitants operating simultaneously, neither of which would have been addressed by lactulose alone.
Identifying and Treating the Precipitant: The Step That Changes Everything
Lactulose will not fix an untreated GI bleed. Rifaximin will not resolve an untreated urinary tract infection. The single most important step in hepatic encephalopathy management is systematic precipitant identification - because treating the precipitant is what resolves the episode. Ammonia-lowering therapy buys time; precipitant correction ends it.
The common precipitants, in rough order of frequency: GI bleeding, infection (SBP, UTI, pneumonia), electrolyte disturbance (hyponatraemia, hypokalaemia, metabolic alkalosis), renal impairment, constipation, excess dietary protein, sedative or benzodiazepine use, and non-adherence to lactulose or rifaximin.
Systematic bedside approach:
Check for GI bleeding - even low-grade occult bleeding can precipitate HE in a cirrhotic. Examine for melaena, haematochezia, or haematemesis. Consider urgent OGD if suspected.
Screen for infection - blood cultures, urine culture, and diagnostic paracentesis if ascites is present. Do not wait for fever; cirrhotic patients with SBP are frequently afebrile.
Review electrolytes and renal function - hypokalaemia drives renal ammonia production. Creatinine rise signals hepatorenal physiology or dehydration.
Review the medication list - benzodiazepines, opioids, and proton pump inhibitors (via small intestinal bacterial overgrowth) all have known associations with HE precipitation. Rifaximin in cirrhosis reduces recurrence by modulating the gut microbiome - its effect is not simply antibiotic.
Assess diuretic status - overzealous diuresis causes both hyponatraemia and renal impairment, a double precipitant hit.
Per current AASLD guidance, all identified precipitants should be treated concurrently with ammonia-lowering therapy - not sequentially.
A Frequently Overlooked Point: Zinc, Sarcopenia, and Recurrent HE
Clinicians who manage frequent HE relapsers often focus exclusively on lactulose adherence and rifaximin compliance. What frequently escapes attention is the role of muscle mass as an ammonia buffer. Skeletal muscle is the primary extrahepatic site of ammonia metabolism - and cirrhotic patients with sarcopenia lose this buffer progressively. Zinc deficiency, present in up to 70% of cirrhotics, impairs the urea cycle and further reduces ammonia clearance. In patients with recurrent HE despite adequate lactulose and rifaximin, checking serum zinc and supplementing where deficient (typically 220 mg zinc sulphate twice daily) is a low-risk, evidence-supported adjunct. Nutritional optimisation - specifically late evening snack with branched-chain amino acids - reduces HE recurrence independently of pharmacotherapy.
Bottom Line for Clinical Practice
Grade HE clinically, not biochemically. Ammonia guides suspicion - the West Haven Criteria grade the patient.
Always perform diagnostic paracentesis in any HE episode with known ascites - SBP is a precipitant in up to 35% of HE admissions and is frequently asymptomatic.
Lactulose target is 2–3 soft stools per day - not as many stools as possible. Over-purgation causes dehydration and electrolyte disturbance, which become new HE precipitants.
Add rifaximin 550 mg twice daily for secondary prevention in any patient with a second overt HE episode - the Bajaj et al. RCT (Hepatology 2018) demonstrated a 58% reduction in HE recurrence over lactulose alone.
In grade III–IV HE, protect the airway actively. Do not assume the patient will maintain it. Early ICU liaison and anaesthetic review is appropriate before deterioration forces an emergency intubation.
When your next HE patient arrives - confused, somnolent, or somewhere in between - use GastroAGI to walk through the grading, run the precipitant checklist, and generate a management sequence anchored to their specific clinical picture. It will not replace your clinical judgement, but it will make sure nothing important is missed.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.