15/07/2026
0viewsMaddrey's Discriminant Function: Deciding Steroid Candidacy in Alcohol-Associated Hepatitis
Maddrey's discriminant function decides steroid candidacy in alcoholic hepatitis, not survival alone. How to calculate it, when it misleads, and what to check next.
Quick Answer
Maddrey's discriminant function decides steroid candidacy in alcoholic hepatitis, not survival alone. How to calculate it, when it misleads, and what to check next.
A 47-year-old man with a 20-year history of heavy drinking is admitted with new jaundice, a total bilirubin of 9.8 mg/dL, and a prothrombin time nine seconds above control. He has no ascites, no encephalopathy, and no signs of active bleeding. The team's first question isn't whether he has alcoholic hepatitis - the history and labs already answer that. The question is whether he needs prednisolone, and Maddrey's discriminant function is the number that answers it.
Maddrey's discriminant function was never built to predict who lives and who dies from alcohol-associated hepatitis in general. It was built for one narrower, more useful purpose: identifying which patients had enough to gain from corticosteroid therapy that the risk was worth taking. That distinction gets lost constantly on the wards, where a DF gets calculated, filed as "severe," and used loosely as a catch-all severity marker instead of what it actually is - a steroid-eligibility gate with a single, specific cutoff. Clinicians who treat it as a general prognostic score end up either under-treating patients who clear the threshold or, more often, anchoring on a DF above 32 as sufficient justification for steroids without checking the contraindications that make that decision reversible. The formula itself is simple; using it correctly is not.
Calculating Maddrey's Discriminant Function Correctly
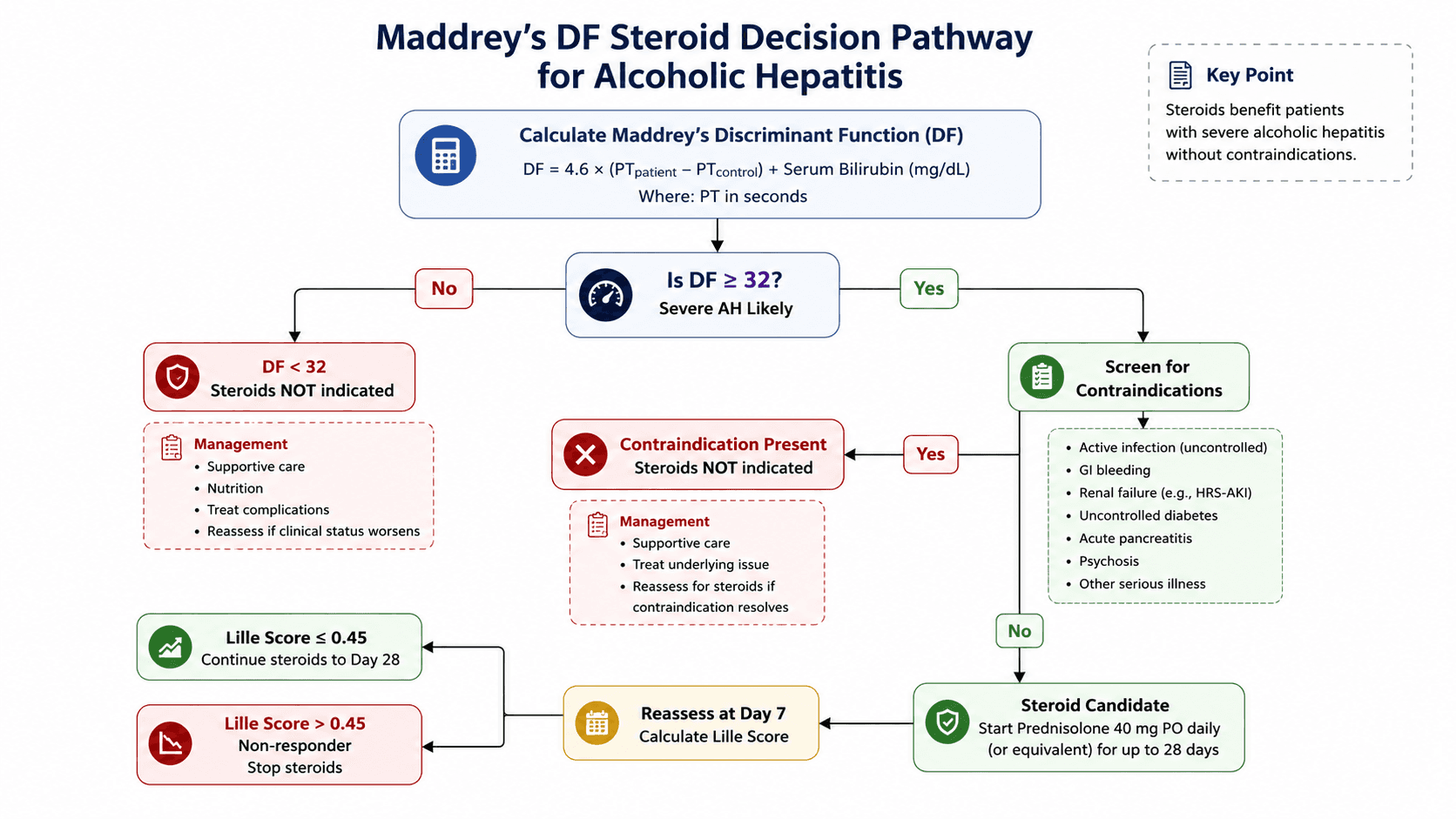
The formula is DF = 4.6 × (patient prothrombin time − control prothrombin time, in seconds) + total serum bilirubin (mg/dL). Both inputs sound straightforward, and both are where errors creep in.
The control prothrombin time is not standardized across labs, and a higher control value systematically lowers the calculated DF - meaning the same patient can cross or miss the treatment threshold depending on which reference range a hospital lab uses. This is not a theoretical concern; retrospective data have shown that the choice of control PT measurably changes how often clinicians offer steroids, without changing the underlying disease. Confirm your institution's current control PT before trusting a borderline result, and recalculate if a patient is transferred between systems using different reference values.
Total bilirubin should be the most recent value, not an admission value if several days have passed - AH can progress quickly, and a DF calculated on stale labs can understate current severity. A DF of 32 or higher is the conventional threshold established in the original McCullough and O'Connor criteria and defines severe alcoholic hepatitis. Below 32, corticosteroids are not indicated regardless of how sick the patient otherwise appears; the mortality benefit steroids offer has only been demonstrated in the severe subgroup.
Have you checked out the Free Maddreys DF Calculator?

Case in point
A 52-year-old woman presents with a DF of 38, no infection on screening cultures, and no gastrointestinal bleeding. Per guideline-directed care, she starts prednisolone 40 mg daily. Her bilirubin is rechecked on day 7, and her Lille score comes back at 0.31 - a responder, meaning bilirubin trended down enough to justify completing the full 28-day course.
Contrast that with a 61-year-old man, also with a DF of 38, who is found to have a low-grade urinary tract infection on admission labs. The infection is treated first, and only once source control is confirmed does the team revisit steroid candidacy - DF alone does not override an active, untreated infection as a contraindication. This is the operational reality of Maddrey's DF: it opens the door to a treatment decision, but it does not close the loop on patient selection by itself. Sepsis, active variceal bleeding, and renal failure all modify whether a DF-eligible patient should actually receive steroids that day.
Where Maddrey's DF Falls Short - and What to Check Next
The STOPAH trial, the largest randomized study of alcoholic hepatitis treatment to date, found that a DF of 32 or higher did not reliably separate patients who benefited from prednisolone from those who didn't. Patients with a Glasgow Alcoholic Hepatitis Score (GAHS) above 8, in the absence of sepsis or GI bleeding, showed a more consistent treatment response than DF-based selection alone predicted. This doesn't mean DF is obsolete - it remains the standard trial-inclusion criterion and the number most guidelines still reference - but it means a DF just above 32 shouldn't be read as a confident, isolated treatment signal. Recalculating GAHS alongside DF gives a second, complementary check before committing a borderline patient to a month of corticosteroids with real risk of infection, hyperglycemia, and GI bleeding.
The other half of correct DF use happens after treatment starts, not before. A baseline DF only tells you whether to start steroids. Whether to continue them is a separate question, answered by the Lille score at day 4 or day 7, which incorporates the bilirubin trend on treatment rather than a single admission snapshot. A Lille score above 0.45 identifies non-responders, in whom continuing prednisolone offers no survival benefit and only accumulates infection risk. Treating DF as a one-time gate and Lille as the ongoing checkpoint keeps the decision-making sequence in the right order.
A frequently overlooked point
The most common error isn't miscalculating DF - it's stopping the workup once DF clears 32. A discriminant function above the threshold confirms eligibility for steroids; it says nothing about whether the patient has an occult infection that makes steroids dangerous, whether renal function is deteriorating in a pattern consistent with hepatorenal syndrome, or whether the diagnosis is even correct. Alcoholic hepatitis is a clinical diagnosis, and a DF calculated on a patient whose jaundice actually stems from choledocholithiasis or drug-induced liver injury is a number computed on the wrong condition entirely. Before treating a DF as decision-grade, confirm the diagnostic gestalt still fits - recent heavy intake, AST: ALT ratio typically above 1.5 to 2, AST rarely above 400, and imaging that doesn't point to an alternative biliary or infiltrative process.
Bottom line for clinical practice
Use DF ≥ 32 as the threshold for considering corticosteroids in alcoholic hepatitis, not as a general severity or mortality score.
Confirm your institution's control prothrombin time before trusting a DF near the cutoff - a different reference range can move a patient across the treatment threshold.
Rule out sepsis, active GI bleeding, and uncontrolled renal failure before starting steroids, even in a clearly DF-eligible patient.
Recalculate GAHS in borderline cases; STOPAH data suggest it selects steroid responders more precisely than DF alone.
Reassess with the Lille score at day 4–7 on treatment - a poor Lille response means stopping steroids regardless of the starting DF.
Next time a jaundiced patient with a heavy drinking history lands on your service, run the labs through GastroAGI - it will calculate Maddrey's DF alongside GAHS and Lille, and walk through the guideline-anchored reasoning for steroid candidacy in seconds.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.