09/07/2026
18viewsMASLD Onset Age and Type 2 Diabetes Risk: Why Earlier Fatty Liver May Matter More
Earlier MASLD onset may signal higher future type 2 diabetes risk, highlighting the need for earlier metabolic risk assessment.
Quick Answer
Earlier MASLD onset may signal higher future type 2 diabetes risk, highlighting the need for earlier metabolic risk assessment.
Introduction
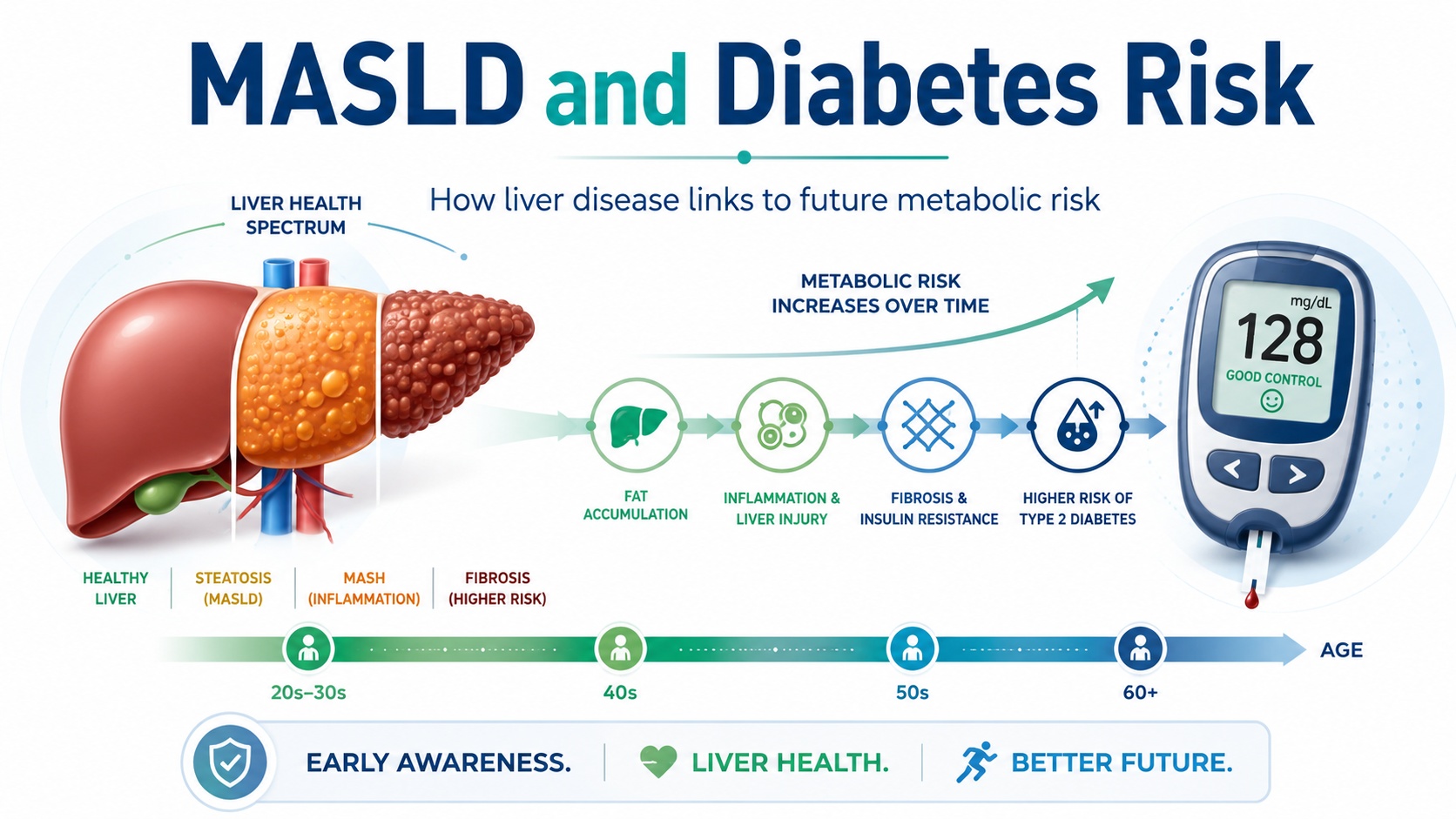
Metabolic dysfunction-associated steatotic liver disease, or MASLD, is no longer viewed as an isolated liver condition. It is increasingly understood as part of a broader metabolic disease network involving obesity, insulin resistance, dyslipidemia, hypertension, cardiovascular risk, and type 2 diabetes.
A new article in Clinical Gastroenterology and Hepatology examines an important and clinically intuitive question: does the age at which MASLD begins influence the future risk of type 2 diabetes?
The study, titled “Association of metabolic dysfunction-associated steatotic liver disease onset age with risk of incident type 2 diabetes,” was published by Huo and colleagues in 2026. The available PubMed-indexed conclusion reports that MASLD onset at any age was associated with increased risk of type 2 diabetes, with earlier onset conferring progressively greater risk.
This is not just an epidemiologic detail. For gastroenterologists and hepatologists, it raises a practical question: should younger patients with MASLD be treated as a higher-risk metabolic group even before diabetes develops?
Why this update matters
MASLD is common, often silent, and frequently detected incidentally on ultrasound, CT, MRI, or abnormal liver enzymes. ACG describes MASLD as fat buildup in the liver in people with diabetes, obesity, hypertension, or high cholesterol who drink little to no alcohol; it also notes that up to 30% of American adults may have MASLD.
AGA similarly describes MASLD as one of the most common causes of liver disease in the United States, affecting an estimated 30–40% of adults.
The clinical challenge is that MASLD is not only about liver fat. It is a marker of systemic metabolic dysfunction. ACG notes that people with MASLD are at risk for diabetes and heart disease, and that heart disease is the leading cause of death among people with MASLD.
This new study adds another layer: timing may matter. A patient who develops MASLD in early adulthood may carry a longer cumulative period of hepatic and systemic metabolic stress than someone who develops MASLD later in life. That longer exposure window could help explain why earlier onset may be associated with greater future diabetes risk.
What the study found
The central finding is straightforward: MASLD onset at any age was associated with increased risk of incident type 2 diabetes, and the association appeared stronger when MASLD began earlier in life.
Because this is an observational study, the key word is association. The study does not prove that MASLD directly causes diabetes. However, the finding is biologically plausible. MASLD and type 2 diabetes share core mechanisms, including insulin resistance, excess adiposity, metabolic inflammation, altered lipid handling, and cardiometabolic risk clustering.
The study is particularly useful because it shifts attention from the binary question “Does this patient have MASLD?” to a more nuanced question: “When did this patient develop MASLD, and how long have they been metabolically exposed?”
That distinction may become increasingly important as younger adults, and even adolescents, present with obesity-related liver disease and metabolic risk factors.
Clinical interpretation
For clinicians, the most useful interpretation is not that MASLD onset age should immediately become a formal risk score by itself. Rather, MASLD onset age may help identify patients who deserve earlier and more deliberate metabolic surveillance.
A 32-year-old with MASLD is not simply a younger version of a 68-year-old with MASLD. The younger patient may face decades of future metabolic risk, including type 2 diabetes, cardiovascular disease, progressive liver fibrosis, and kidney disease. Earlier onset may represent a longer cumulative exposure to insulin resistance and metabolic dysfunction.
This also reinforces the need for multidisciplinary care. MASLD should prompt hepatology evaluation when fibrosis risk is elevated, but it should also trigger metabolic risk assessment. That includes checking glycemic status, lipids, blood pressure, waist or weight trajectory, cardiovascular risk factors, and family history.
AGA’s MASLD toolkit highlights the importance of clinical care pathways that integrate noninvasive fibrosis risk stratification and management resources for patients with MASLD and MASH. AASLD also maintains practice guidance resources for MASLD assessment and management, emphasizing evidence-based approaches to diagnostic, therapeutic, and preventive care.
Practical implications for gastroenterologists
For gastroenterologists, this study supports a more proactive approach when MASLD is identified at a younger age.
First, document the age or approximate time of MASLD onset whenever possible. Many patients are told they have “fatty liver” years before they reach specialist care. That history may matter.
Second, screen for glycemic abnormalities. A normal fasting glucose at one visit should not create false reassurance in a young patient with MASLD, obesity, dyslipidemia, or family history of diabetes. HbA1c and fasting glucose should be followed longitudinally, with consideration of broader metabolic evaluation when clinically appropriate.
Third, assess fibrosis risk. Diabetes risk matters, but liver risk still matters. Patients with MASLD should be risk-stratified for advanced fibrosis using noninvasive tools such as serum-based scores, elastography, or other validated pathways when appropriate.
Fourth, counsel early. Younger patients may have the greatest opportunity for long-term risk modification. Lifestyle intervention, weight management, physical activity, improved sleep, reduced sugar-sweetened beverage intake, and cardiometabolic optimization are more valuable when implemented before diabetes develops.
Fifth, coordinate care. MASLD often sits between gastroenterology, hepatology, endocrinology, cardiology, primary care, and nutrition. Earlier-onset MASLD may be a strong reason to build shared-care pathways rather than manage the liver finding in isolation.
Limitations and caution
This study should be framed carefully. It is observational, so it cannot prove causality. Earlier MASLD onset may be a marker of more severe or longer-standing metabolic dysfunction rather than an independent causal driver of diabetes.
There may also be confounding by body weight, genetics, diet, socioeconomic factors, physical activity, medication exposure, family history, and baseline insulin resistance. The full article should be reviewed for study population, MASLD definition, diabetes ascertainment, adjustment variables, subgroup analyses, and sensitivity analyses before translating the findings into formal protocols.
Another limitation is practical: in real-world care, the exact onset age of MASLD is often uncertain. Many patients are asymptomatic, and liver fat may be detected only when imaging is performed for unrelated reasons. Therefore, “onset age” may sometimes mean “age at detection,” not true biological onset.
GastroAGI takeaway
This study strengthens a clinically important message: MASLD is not just a liver imaging finding. It is a metabolic risk signal.
The key takeaway is that earlier MASLD onset may identify patients at progressively higher risk of developing type 2 diabetes. For gastroenterologists and hepatologists, that means younger patients with MASLD should not be reassured solely because they are young. Instead, they may deserve earlier metabolic screening, longitudinal glycemic follow-up, fibrosis risk assessment, and coordinated lifestyle and cardiometabolic intervention.
This is not yet a practice-changing trial. But it is a clinically useful reminder that in MASLD, timing matters.
Reference / Source
Huo Z, Li Y, Liu T, et al. Association of metabolic dysfunction-associated steatotic liver disease onset age with risk of incident type 2 diabetes. Clinical Gastroenterology and Hepatology. 2026. DOI: 10.1016/j.cgh.2026.06.028.
Key Points
MASLD onset at any age was associated with increased risk of incident type 2 diabetes.
Earlier MASLD onset appeared to confer progressively greater diabetes risk.
MASLD should be viewed as a systemic metabolic risk marker, not only a liver condition.
Younger patients with MASLD may need earlier and more consistent glycemic surveillance.
The study is observational, so it supports risk awareness but does not prove causality.
Clinical management should still include fibrosis risk stratification, lifestyle intervention, and cardiometabolic optimization.
The strongest GastroAGI angle: “In MASLD, age of onset may help identify who needs earlier diabetes prevention attention.”
Explore GastroAGI
If you are a gastroenterologist, trainee, researcher, or medical educator navigating journals, guidelines, conferences, and clinical questions every day, GastroAGI is built for you.
GastroAGI brings GI-focused intelligence into one structured platform — helping users learn, reason, and communicate with more clarity across Student, Clinician, and Patient modes.
Explore how specialized AI can support modern gastroenterology workflows.
Visit GastroAGI: https://gastroagi.com
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.