09/07/2026
35viewsMELD-Na Score: How to Interpret It and When It Changes the Transplant Conversation
MELD-Na score interpretation: what the numbers mean, when hyponatremia changes transplant priority, and how it compares to Child-Pugh. Calculate yours instantly.
Quick Answer
MELD-Na score interpretation: what the numbers mean, when hyponatremia changes transplant priority, and how it compares to Child-Pugh. Calculate yours instantly.
A 58-year-old woman with alcohol-related cirrhosis is admitted for worsening ascites. Her creatinine and INR are stable compared to three months ago, and on a quick glance, her chart looks unremarkable. Her sodium, though, has dropped from 135 to 128 mEq/L over that same window. Her MELD score barely moved. Her MELD-Na score jumped six points. The transplant team's tone in the room changed before the labs were even fully explained to the family - and that shift, the gap between what MELD says and what MELD-Na says, is exactly what this post walks through.
Why sodium changes the conversation
The original MELD score - bilirubin, INR, creatinine - was built to predict short-term mortality after TIPS placement and was later adopted for liver-transplant waitlist prioritization. It works well for most patients. But a subset of cirrhotic patients decompensate with a pattern the original three variables miss entirely: dilutional hyponatremia from advanced portal hypertension and sustained neurohormonal activation, occurring even when synthetic liver function looks relatively preserved on paper. The MELD-Na score added serum sodium specifically because hyponatremia independently predicts waitlist mortality, and a patient can look stable on MELD while their true risk of dying before transplant is climbing underneath that stability.
This is the gap clinicians repeatedly fall into: trusting a flat MELD trend across visits without separately checking whether sodium is telling a different story. It's an easy gap to fall into precisely because bilirubin, INR, and creatinine are the labs everyone reflexively scans first, while sodium sits lower on the panel and gets mentally filed under "electrolytes," not "prognosis." Anyone using the MELD-Na calculator day to day already knows the number moves faster than intuition expects once sodium drops below 130 - and that gap between what MELD says and what MELD-Na says is often the first real signal that a patient's trajectory has shifted.
What the MELD-Na number is actually telling you
MELD-Na is calculated from the standard MELD score with a sodium correction applied once serum sodium falls between 125 and 137 mEq/L - values outside that range are capped at the boundary rather than extrapolated further. The correction isn't linear intuition; a patient at MELD 15 with sodium 126 can end up with a MELD-Na in the low 20s, a difference that meaningfully changes waitlist position and, in a borderline case, the urgency of the entire transplant conversation.
Per OPTN/UNOS allocation policy, MELD-Na is the score actually used for adult liver-transplant waitlist prioritization in the United States, not raw MELD. The landmark trial behind this, Kim et al. (NEJM, 2008), followed over 7,000 waitlisted patients and found that for any given MELD score, waitlist mortality rose substantially as sodium fell - patients with sodium under 125 had markedly worse 90-day survival than their MELD score alone predicted. That finding is why sodium correction exists at all: MELD systematically underestimated risk in the hyponatremic subgroup, and MELD-Na closed most of that gap. It's worth remembering this wasn't a marginal statistical refinement - it was large enough to change national organ allocation policy.
The practical implication is that a patient with refractory ascites requiring frequent large-volume paracentesis, or one on chronic diuretics who develops progressive hyponatremia, deserves a MELD-Na recheck even if bilirubin and INR haven't moved since the last visit. Sodium drift is often the earliest signal of worsening effective arterial blood volume and sustained neurohormonal decompensation, well before the other three variables catch up to reflect the same underlying deterioration. Waiting for bilirubin or creatinine to confirm what sodium already suggested means acting on the lagging indicator instead of the leading one.
Case in point
A 61-year-old man with hepatitis C-related cirrhosis, now cured virologically, presents with increasing abdominal girth over six weeks. His bilirubin is 1.8 mg/dL, INR 1.3, creatinine 0.9 mg/dL - a MELD of 11, unremarkable and essentially unchanged from his visit four months earlier. His sodium, however, has fallen to 127 mEq/L on a routine outpatient panel, driven by a combination of low-salt intake inconsistency, recent diuretic escalation for worsening ascites, and progressive portal hypertension that his imaging had already started to hint at.
Recalculating with sodium correction, his MELD-Na comes out to 18 - a seven-point jump that would not have been obvious from the MELD trend alone, and one that moved him from a score most clinics wouldn't flag urgently to one that changes the referral timeline. That gap prompted an earlier transplant-center referral than his MELD score in isolation would have triggered, along with a fluid-restriction and diuretic-adjustment conversation that his prior visits hadn't flagged as urgent. Six weeks later, a repeat outpatient panel showed sodium recovering to 132 with adjusted diuretic dosing - a reminder that MELD-Na, unlike a one-time risk label, is meant to be tracked, not filed away after a single calculation.
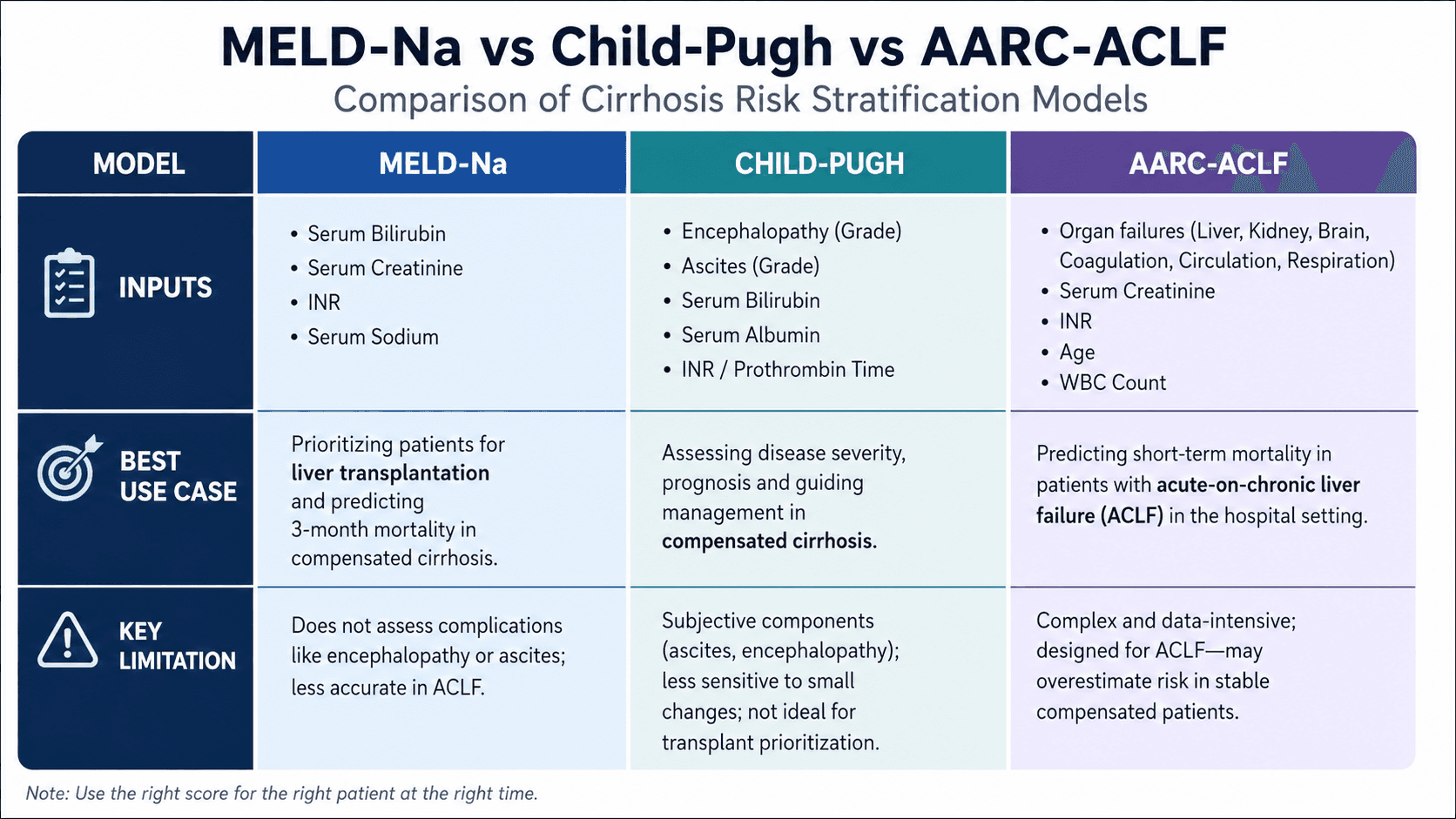
Where MELD-Na fits against the other tools on the shelf
MELD-Na isn't competing with Child-Pugh so much as complementing it, and conflating the two is a common source of miscommunication on rounds. Child-Pugh remains useful for surgical risk stratification and is still referenced in some non-transplant contexts, but it relies on subjective inputs - ascites and encephalopathy graded clinically rather than measured - and has a narrower discriminatory range at the sicker end of the spectrum, where most transplant-timing decisions actually happen. MELD-Na, built entirely from objective lab values, tends to separate high-acuity patients more precisely, which is exactly the population where a few points of score difference change real outcomes.
The distinction matters even more once a patient develops acute-on-chronic liver failure, where a single static MELD-Na snapshot stops being sufficient on its own - that's the scenario the AARC-ACLF score was built for, incorporating the trajectory of organ failure over the first week rather than a single point-in-time value. A patient with a moderate MELD-Na who is rapidly accumulating organ failures needs a different urgency assessment than the number alone conveys, and AARC-ACLF is the tool designed to capture exactly that.
Similarly, in a patient presenting with alcohol-associated hepatitis specifically, treatment candidacy still runs through Maddrey's discriminant function, not MELD-Na - Maddrey's DF is what determines whether corticosteroid therapy is indicated, a decision MELD-Na alone was never designed to answer. Knowing which score answers which clinical question, rather than defaulting to whichever number is most familiar, is as important as calculating any single one of them correctly.
A frequently overlooked point
Clinicians often recalculate MELD-Na only at scheduled transplant re-evaluation intervals, treating it as an administrative checkpoint rather than a live clinical signal that deserves attention whenever new labs come in. That habit misses the patients who decompensate between visits - the ones with a slow sodium drift on a routine metabolic panel drawn for an unrelated reason, that nobody flagged because bilirubin and creatinine looked fine and the ordering physician wasn't thinking about transplant listing at all. A same-day recheck any time sodium falls below 130 in a known cirrhotic patient, regardless of why the labs were originally drawn, catches this earlier than waiting for the next scheduled reassessment. In practice, this means the primary care physician managing a cirrhotic patient's diuretics needs to know that a routine sodium of 128 is not just an electrolyte abnormality to correct - it's a prognostic signal that belongs in the hepatology team's inbox that same day.
Bottom line for clinical practice
Recalculate MELD-Na whenever serum sodium drops below 130 mEq/L in a cirrhotic patient, even if bilirubin, INR, and creatinine are unchanged.
Remember the sodium correction only applies between 125–137 mEq/L - values outside this range are capped, not extrapolated.
MELD-Na, not raw MELD, is the score used for actual U.S. liver-transplant waitlist prioritization under current OPTN policy.
In acute-on-chronic liver failure, layer in AARC-ACLF rather than relying on a single MELD-Na value to capture trajectory.
For alcohol-associated hepatitis specifically, treatment candidacy still runs through Maddrey's DF, not MELD-Na.
Next time a cirrhotic patient's labs look stable but something still feels off, run the numbers through GastroAGI - it will flag exactly this kind of sodium-driven MELD-Na shift and walk through the guideline-anchored reasoning behind it in seconds.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.