18/05/2026
7viewsObesity Pharmacotherapy in 2026: How EASO's Complication-First Framework Changes the Way You Choose a Drug
EASO 2026 shifts obesity drug selection from BMI to complication: here's how tirzepatide, semaglutide, and others map to MASLD, HF, OSAS, and T2DM
Quick Answer
EASO 2026 shifts obesity drug selection from BMI to complication: here's how tirzepatide, semaglutide, and others map to MASLD, HF, OSAS, and T2DM

Your patient has a BMI of 34, MASLD on ultrasound, and an HbA1c of 6.8%. You reach for a GLP-1 - but which one? For what endpoint? And what counts as treatment success? Until recently, the default answer was "the one that causes the most weight loss." The EASO 2026 framework formally dismantles that logic.
For years, obesity pharmacotherapy was weight-loss pharmacotherapy. The primary endpoint was kilograms - and the drug hierarchy followed suit. That framing missed something fundamental: the patient sitting across from you doesn't have "obesity." They have sleep apnoea worsening their hypertension, or knee pain preventing them from exercising, or steatohepatitis quietly progressing toward cirrhosis. The EASO 2026 update on obesity pharmacotherapy makes explicit what many experienced clinicians already suspected - the right drug depends entirely on the complication you are trying to reverse, not on BMI alone.
This reframing matters particularly for gastroenterologists and hepatologists. Obesity is not a background variable in MASLD, MASH, or metabolic-associated liver disease. It is often the primary driver. The 2026 framework now positions liver disease endpoints - MASH remission and fibrosis improvement - as legitimate treatment targets for obesity-management medication (OMM), with drug-specific evidence mapped to each endpoint.
The Mechanical vs Metabolic Divide: Why Your Endpoint Changes Everything in Obesity Pharmacotherapy
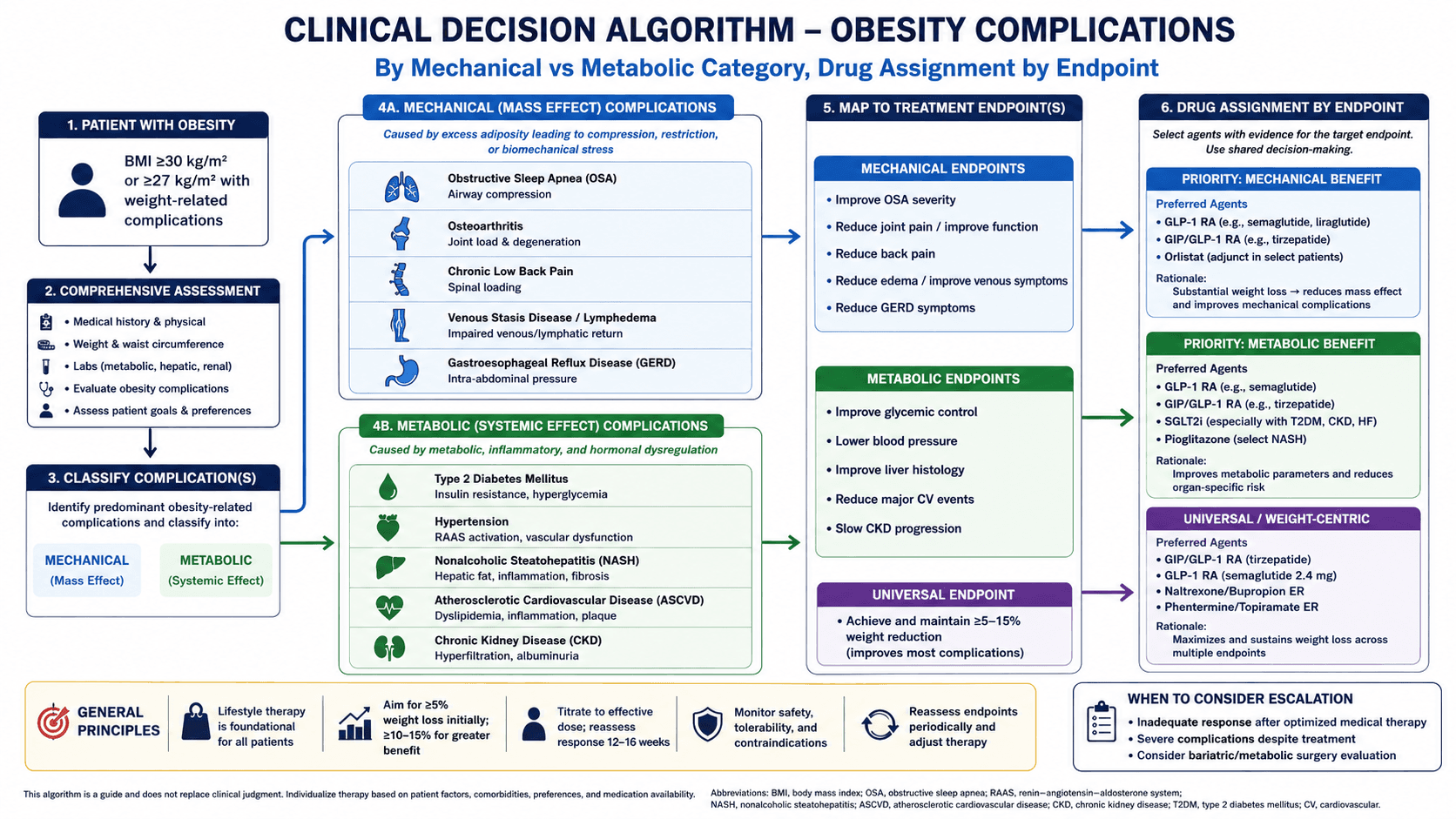
The EASO 2026 framework divides obesity complications into two mechanistic categories, and this division is clinically operational - not just taxonomic.
Mechanical adiposity refers to complications driven by excess physical mass: obstructive sleep apnoea syndrome (OSAS) from pharyngeal fat deposition and reduced chest wall compliance, and knee osteoarthritis (KOA) from increased joint load. The treatment target here is mechanical unloading - weight loss that reduces physical forces. In OSAS, the goal is remission; in KOA, it is pain remission and improved mobility.
Metabolic adiposity covers the broader cardiometabolic and hepatic spectrum: prediabetes, type 2 diabetes, atherosclerotic cardiovascular disease, heart failure with preserved ejection fraction, MASLD, MASH, and liver fibrosis. Here the pathophysiology involves adipokine dysregulation, ectopic fat deposition, insulin resistance, systemic inflammation, and direct lipotoxicity. Weight loss helps - but the ideal drug also targets the tissue-level pathology, not only the scale.
Per the EASO 2026 update, the clinical question to ask before prescribing is no longer "What is the BMI?" but "What complication am I treating, and what endpoint defines success?" This is a structural shift in how obesity is managed - from a single-axis disorder to a complication-specific disease requiring the same endpoint-driven logic as hypertension or dyslipidaemia.
The drug hierarchy follows directly from this. Tirzepatide leads for total body weight loss. Semaglutide has the broadest complication-specific evidence across cardiovascular disease (MACE reduction via SELECT), MASLD/MASH, prediabetes, knee OA, heart failure, and - crucially - liver fibrosis improvement. These are not interchangeable drugs prescribed for interchangeable reasons.
Clinical Scenario: MASLD with Obesity - When "Lose Weight" Is Not a Complete Order
A 51-year-old woman presents with a 3-year history of MASLD on ultrasound. Her BMI is 33.4. She has prediabetes (HbA1c 6.4%), mild dyslipidaemia, and no prior cardiovascular events. Her liver stiffness on FibroScan is 7.2 kPa. She has tried lifestyle modification twice - each time losing 6–8 kg and regaining it within a year.
She is started on semaglutide 2.4 mg weekly, with the explicit treatment targets stated at initiation: normalisation of glycaemia, liver enzyme improvement, and - as fibroscan is repeated at 12 months - a reduction in liver stiffness as a proxy for fibrosis regression. At 14 months, HbA1c is 5.7%, she has lost 11% total body weight, and her liver stiffness has decreased to 5.8 kPa.
The distinction here matters operationally. If weight loss alone were the endpoint, a 10% reduction might be framed as a partial success. Framed instead as MASH remission and fibrosis stabilisation in a patient at risk of progression, it is a clinically meaningful disease-modifying outcome - and it changes how you counsel the patient on long-term continuation.
Read more about NAFLD & MASH Treatment: https://gastroagi.com/blog/nafld-nash-treatment-resmetirom
Semaglutide, Tirzepatide, and the Rest: Mapping Drug Evidence to Liver and Cardiometabolic Endpoints
For gastroenterologists, the liver-specific evidence is now actionable. The EASO 2026 framework identifies semaglutide as the drug with current evidence for both MASH remission and liver fibrosis improvement - the latter categorised explicitly as a 2026 update, reflecting emerging data from the NASH trials and the ESSENCE trial programme. Tirzepatide, despite its superior weight-loss efficacy, does not yet carry mapped evidence for the fibrosis endpoint in the EASO framework.
This has a practical implication: in a patient with obesity and biopsy-proven or fibroscan-confirmed significant fibrosis (≥F2), semaglutide at obesity dosing (2.4 mg weekly) is the better-evidenced choice at present - even if tirzepatide might produce greater weight loss. The treatment target is the liver, not the scale.
For the cardiovascular endpoint (MACE reduction), semaglutide again holds the evidence - the SELECT trial demonstrated a 20% reduction in MACE in patients with obesity and established cardiovascular disease, without diabetes as an entry requirement. This was a landmark shift: cardiovascular protection from an obesity drug independent of glycaemic benefit.
Tirzepatide leads for total body weight loss (SURMOUNT-1: ~20% TBWL at 72 weeks) and has emerging evidence for OSAS remission, making it the preferred agent when maximal weight reduction is the dominant goal - particularly in patients with severe obesity, high surgical risk, or those being optimised prior to bariatric procedures. For heart failure, both tirzepatide (SUMMIT) and semaglutide carry evidence for hospitalisation reduction in obese HFpEF patients - a population that represents a growing proportion of heart failure admissions in South Asian practices.
Liraglutide remains relevant at 3 mg daily, particularly for knee osteoarthritis pain remission and as a lower-cost incretin option in prediabetes - but it is no longer the leading agent for most metabolic endpoints. Older agents (orlistat, naltrexone-bupropion, phentermine-topiramate) retain narrower roles: phentermine-topiramate contributes to weight loss but lacks complication-specific evidence for most organ endpoints.
A Frequently Overlooked Point: Framing the Endpoint Before You Write the Prescription
The most underused step in obesity pharmacotherapy is stating the treatment target explicitly before initiating the drug - not to the patient's BMI, but to their dominant complication. This matters because it defines what success looks like at 6 months, determines when to escalate or switch, and - critically - strengthens the clinical justification for long-term continuation in systems where cost or formulary access requires documented medical necessity.
A patient whose treatment goal is "MASH remission and fibrosis stabilisation" has a different monitoring plan (LFTs, fibroscan, MRE at 12 months) than a patient whose goal is "MACE risk reduction" (lipid panel, blood pressure, event-free survival). Both may be on semaglutide. Both are treated for obesity. The drug is the same; the clinical logic is not.
Bottom Line for Clinical Practice
Do not anchor drug selection to BMI alone. The EASO 2026 framework requires identifying the dominant complication first - MASLD/MASH, cardiovascular disease, heart failure, OSAS, prediabetes, or T2DM - and selecting the agent with outcome evidence for that endpoint.
For MASH remission and liver fibrosis improvement, semaglutide currently has the strongest mapped evidence. Tirzepatide produces superior weight loss but lacks equivalent fibrosis endpoint data in the 2026 framework.
For MACE reduction in obesity without diabetes, semaglutide is the drug with trial evidence - the SELECT trial established this independently of glycaemic benefit.
Tirzepatide leads for total body weight loss and is the preferred agent when maximal weight reduction is the primary goal - including pre-bariatric optimisation or severe obesity with OSAS.
State the treatment target explicitly at initiation - endpoint, monitoring interval, and definition of response. This changes counselling, follow-up planning, and the case for long-term continuation.
When your next patient with MASLD and obesity sits across from you, the question is no longer which drug helps them lose the most weight. It is which drug best targets their liver - and what endpoint confirms it is working. GastroAGI can walk through the clinical details with you in real time: complication profile, drug mapping, monitoring intervals, and the evidence behind each decision.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.