10/07/2026
20viewsRisk-Based Follow-Up After HCC Ablation: Toward Smarter Surveillance After Curative Therapy
A new JHEP Reports study explores risk-based follow-up after HCC ablation to personalize recurrence surveillance after curative therapy.
Quick Answer
A new JHEP Reports study explores risk-based follow-up after HCC ablation to personalize recurrence surveillance after curative therapy.
Introduction
Hepatocellular carcinoma, or HCC, remains one of the most recurrence-prone cancers managed by hepatologists, gastroenterologists, interventional radiologists, surgeons, and oncology teams.
For selected patients with early-stage HCC, local ablation can be a curative-intent therapy. However, the clinical challenge does not end once complete ablation is achieved. The next question is just as important: how should these patients be followed after treatment?
A new JHEP Reports article titled “A risk-based post ablation follow-up strategy for hepatocellular carcinoma” addresses this question. The article was available online on July 6, 2026, as an in-press journal pre-proof.
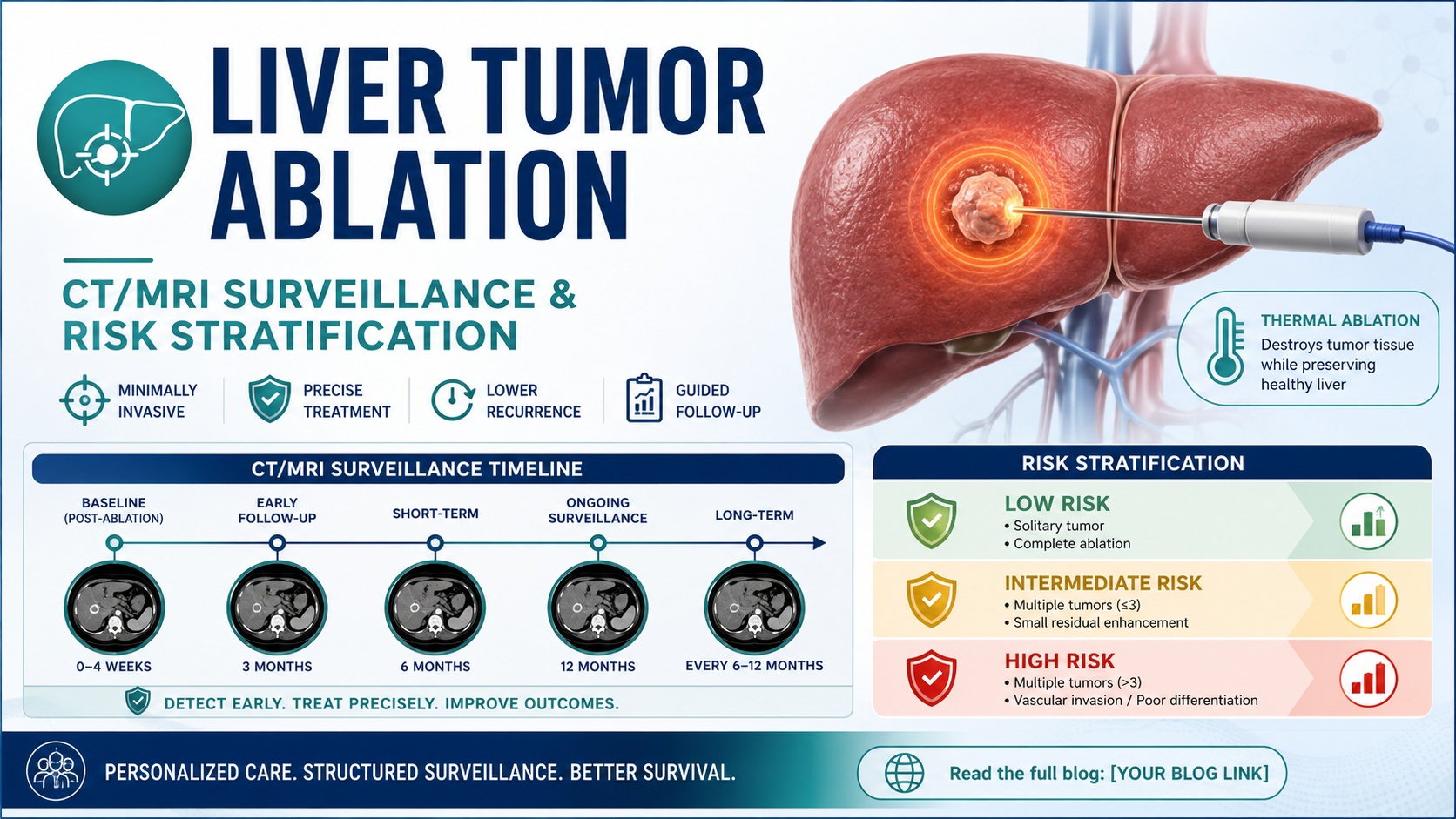
The study is clinically relevant because many HCC follow-up pathways still rely on fixed imaging intervals. The article notes that after ablation, patients were recommended routine follow-up at intervals of 3–6 months during the first 2 years and every 6–12 months thereafter.
That approach is simple, but it may not be optimal for everyone.
Why this update matters
HCC recurrence risk after curative-intent therapy is not uniform. Some patients recur early, some recur late, and some remain recurrence-free for long periods. A fixed follow-up schedule may therefore overtreat lower-risk patients while under-serving patients with higher recurrence risk.
This matters for several reasons.
First, earlier detection of recurrence can preserve the chance of repeat curative-intent therapy, including repeat ablation, resection, transplantation evaluation, or locoregional therapy depending on disease pattern and liver reserve.
Second, repeated CT or MRI surveillance is resource-intensive. It adds cost, patient anxiety, contrast exposure, travel burden, and clinic load.
Third, HCC care is increasingly moving toward individualized decision-making. We already personalize treatment based on tumor stage, liver function, performance status, portal hypertension, transplant eligibility, and multidisciplinary review. Follow-up after ablation should logically move in the same direction.
AASLD maintains HCC practice guidance resources focused on prevention, diagnosis, and treatment, underscoring that HCC care requires evidence-based, multidisciplinary decision-making.
What the study examined
According to the indexed article information, the investigators retrospectively analyzed patients who received complete ablation for initial HCC within the Milan criteria from two tertiary hospitals in China.
The key concept was to move beyond a single fixed schedule and develop a risk-based post-ablation surveillance strategy. In practical terms, this means follow-up intensity could be aligned with estimated recurrence risk rather than applied equally to every patient.
This type of study is important because post-treatment HCC surveillance has to balance two competing goals:
Detect recurrence early enough to act.
Avoid unnecessary imaging and clinic visits in patients whose recurrence risk is relatively lower.
The available source information does not support treating this as a definitive guideline. It is better understood as a risk-stratification and surveillance-optimization study.
Clinical interpretation
The main clinical message is not that current follow-up schedules are wrong. Rather, this study highlights that fixed surveillance intervals may be too blunt for a disease as biologically heterogeneous as HCC.
After ablation, recurrence risk may be influenced by tumor-related factors, liver-related factors, treatment-related factors, and host-related factors. Clinicians commonly consider tumor size, tumor number, AFP, liver function, viral hepatitis status, cirrhosis severity, ablation margin, imaging response, and prior recurrence history when estimating risk.
A risk-based follow-up model could help identify patients who may benefit from closer surveillance early after ablation, when recurrence risk is concentrated. Conversely, patients with lower predicted risk might avoid unnecessary high-frequency imaging, provided safety is maintained.
This is especially relevant in systems where MRI access is limited, CT capacity is strained, or patients travel long distances for surveillance.
The most useful way to frame this update for clinicians is:
HCC surveillance after ablation may eventually become adaptive, not one-size-fits-all.
Practical implications for gastroenterologists and hepatologists
For clinicians managing HCC patients after ablation, this article supports several practical reflections.
First, post-ablation follow-up should begin with confirmation of complete response. Imaging quality and interpretation matter. If the ablation zone is difficult to assess, or if margins are uncertain, the patient may need closer early reassessment.
Second, risk documentation should become routine. Instead of simply writing “follow up in 3 months,” clinicians can document why a patient is considered high, intermediate, or lower risk for recurrence.
Third, surveillance planning should be multidisciplinary. Hepatologists, gastroenterologists, radiologists, interventional radiologists, surgeons, oncologists, and transplant teams may each interpret recurrence risk differently. A shared pathway can reduce variation.
Fourth, risk-based strategies should not reduce vigilance inappropriately. HCC patients often have cirrhosis or chronic liver disease, meaning they remain at risk not only for local recurrence but also for new intrahepatic tumors.
Fifth, patient communication matters. Patients should understand that “less frequent imaging” does not mean less serious care, and “more frequent imaging” does not necessarily mean recurrence is expected. It means surveillance is being matched to risk.
Limitations and caution
This update should be interpreted carefully.
The study is retrospective, which means it can identify patterns and build risk-based strategies, but it cannot prove that a new surveillance schedule improves survival compared with standard care.
The reported study population included patients treated at two tertiary hospitals in China and patients with initial HCC within the Milan criteria. That may limit generalizability to other populations, including patients with non-viral liver disease, different transplant pathways, different imaging access, or different ablation techniques.
Another important limitation is implementation. A risk-based follow-up model is only useful if it is easy to apply, externally validated, clinically interpretable, and safe across diverse settings.
Finally, this should not be viewed as permission to relax follow-up after HCC ablation. Recurrence remains clinically important, and surveillance decisions should still follow local guidelines, tumor board recommendations, liver function assessment, and patient-specific risk.
GastroAGI takeaway
This JHEP Reports study is a timely reminder that HCC follow-up after ablation may need to become more personalized.
The concept is simple but clinically powerful: patients with different recurrence risks may not need identical surveillance schedules.
For now, this is best viewed as hypothesis-generating and practice-informing, not practice-changing. But it points toward a future in which post-ablation HCC surveillance is guided by recurrence risk, resource stewardship, and patient-centered follow-up rather than fixed intervals alone.
The GastroAGI angle is clear:
After curative-intent HCC ablation, the next frontier may be not just better treatment—but smarter surveillance.
Key Points
A new JHEP Reports article proposes a risk-based follow-up strategy after HCC ablation.
The study focused on patients who received complete ablation for initial HCC within the Milan criteria.
Routine follow-up after ablation is often recommended every 3–6 months in the first 2 years and every 6–12 months thereafter.
A fixed schedule may not match the true recurrence risk of every patient.
Risk-based surveillance could help intensify follow-up for higher-risk patients and reduce unnecessary visits for lower-risk patients.
The evidence is retrospective and should not be treated as a new guideline yet.
The strongest GastroAGI angle: HCC surveillance after ablation may be moving from fixed intervals to individualized risk-based care.
Explore GastroAGI
If you are a gastroenterologist, trainee, researcher, or medical educator navigating journals, guidelines, conferences, and clinical questions every day, GastroAGI is built for you.
GastroAGI brings GI-focused intelligence into one structured platform — helping users learn, reason, and communicate with more clarity across Student, Clinician, and Patient modes.
Explore how specialized AI can support modern gastroenterology workflows.
Visit GastroAGI: https://gastroagi.com
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.