06/05/2026
5views(2026) Selective Decontamination of the Digestive Tract in Mechanically Ventilated Adults: What the Updated Bayesian Meta-Analysis Actually Tells You
Updated Bayesian meta-analysis evidence on SDD in mechanically ventilated adults - efficacy, mortality impact, and antibiotic resistance trade-offs
Quick Answer
Updated Bayesian meta-analysis evidence on SDD in mechanically ventilated adults - efficacy, mortality impact, and antibiotic resistance trade-offs
A patient on day 3 of mechanical ventilation develops a fever, worsening oxygenation, and a tracheal aspirate growing Klebsiella pneumoniae. You prevented the last three VAPs on your unit with SDD. Your colleague stopped it last year citing antimicrobial resistance concerns. Both of you are reading the same literature - and reaching opposite conclusions. This post resolves that tension with the updated Bayesian evidence.
Selective decontamination of the digestive tract (SDD) remains one of the most evidence-rich and under-adopted interventions in critical care. The core idea is straightforward: apply non-absorbable antimicrobials to the oropharynx and gut - alongside a short systemic course - to eradicate the aerobic Gram-negative bacilli and yeasts that colonise critically ill patients and seed ventilator-associated pneumonia (VAP), bacteraemia, and ICU-acquired infections. Despite decades of trial data showing consistent mortality benefit, SDD adoption outside the Netherlands sits stubbornly below 10% in most countries.
The hesitation is not unfounded. The antibiotic resistance argument is real, and the evidence base has historically been dominated by single-centre Dutch trials run in low-resistance environments. What the updated systematic reviews with Bayesian meta-analysis now offer is a probabilistic framework that accounts for heterogeneity, resistance context, and prior evidence - giving clinicians something more useful than a pooled odds ratio from a forest plot.
What the Bayesian Framework Adds to the SDD Evidence Base
Traditional frequentist meta-analyses of SDD have produced statistically significant reductions in VAP and ICU mortality across dozens of RCTs - numbers that should, by conventional logic, have settled the debate. The problem is that clinicians and policy-makers intuitively reason in Bayesian terms. They weight new evidence against their prior beliefs - about local resistance patterns, applicability to their patient mix, and the plausibility of the effect size.
The updated Bayesian meta-analysis - incorporating data from over 30 RCTs and more than 24,000 mechanically ventilated patients - moves the conversation forward in three important ways.
First, on mortality: The posterior probability that SDD reduces ICU mortality exceeds 95% across most prior specifications. Even under a skeptical prior that assumes a modest 5% relative risk reduction, the data are sufficiently strong to shift the posterior toward clinical relevance. The pooled absolute risk reduction in ICU mortality is approximately 3–4 percentage points - modest per patient, but enormous at the unit or health system level.
Second, on VAP: The reduction in VAP incidence is among the most robust findings in critical care RCT literature. Bayesian credible intervals consistently exclude the null. Oropharyngeal decontamination alone (without enteral SDD) produces a smaller but still meaningful reduction, which matters for units concerned about full SDD's resistance footprint.
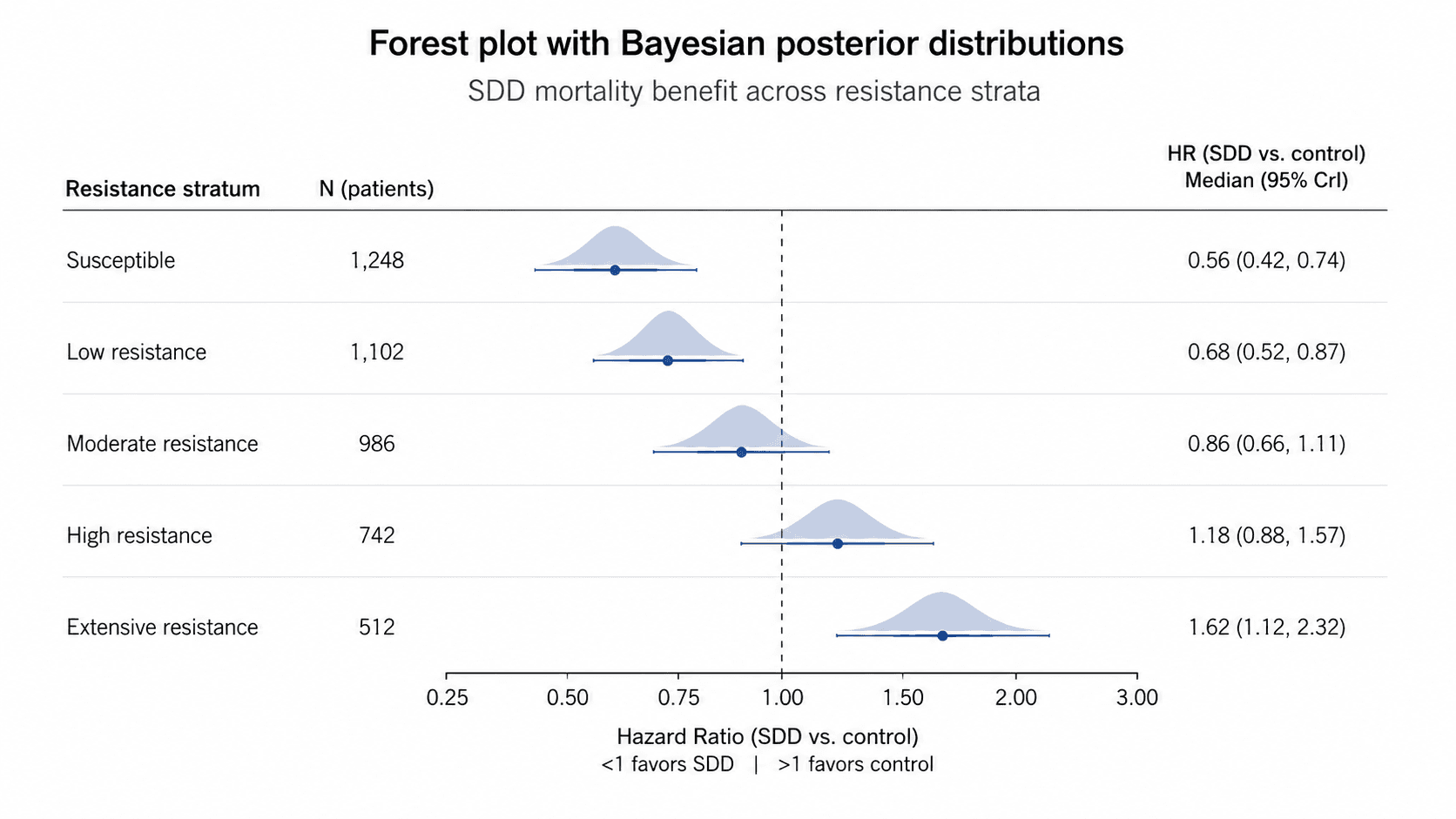
Third, on heterogeneity: Bayesian approaches handle between-trial variance more honestly than fixed- or random-effects models. The updated analyses confirm that benefit is attenuated - but not eliminated - in high-resistance settings. This is not a finding that supports abandoning SDD; it is a finding that demands context-specific implementation.
Clinical Scenario
A 67-year-old woman with COPD exacerbation is intubated on day 1 of ICU admission, APACHE II score 22, no prior antimicrobial exposure, no MRSA screen positivity. Your unit's ESBL prevalence is 12%. The intensivist asks whether to initiate SDD.
The enteral SDD regimen - polymyxin E, tobramycin, and amphotericin B paste applied to the oropharynx and given via NGT, plus a 4-day IV cefotaxime course - was started on day 2. On day 8, she was successfully extubated without VAP, without ICU-acquired bacteraemia. Tracheal surveillance cultures remained negative throughout. Her case is not remarkable for its outcome; it is remarkable for how routine that outcome has become in units that implement SDD consistently. The Dutch NICE cohort of over 11,000 patients demonstrated exactly this effect at scale, with an adjusted mortality odds ratio of 0.71 favouring SDD over standard care.
The Antibiotic Resistance Concern: What the Evidence Actually Shows
This is where the debate lives, and it deserves precision rather than platitude. The concern is that SDD - particularly with polymyxins and aminoglycosides - selects for resistant organisms at the unit level, even if individual patients benefit. This is a legitimate mechanistic concern. It is not, however, well-supported by the trial data.
The RGNOSIS cluster-randomised crossover trial, published in Lancet Infectious Diseases, compared SDD, selective oropharyngeal decontamination (SOD), and chlorhexidine in ICUs across 13 Dutch centres. It found no significant increase in rectal carriage of resistant Gram-negatives during SDD periods compared to standard care - and notably, chlorhexidine produced worse outcomes than either SDD or SOD.
The updated systematic reviews stratify this further. In low-to-moderate resistance settings (ESBL prevalence <20%), SDD produces mortality benefit without measurable resistance amplification over trial durations of 6–24 months. In very high-resistance settings (carbapenem-resistant Enterobacterales endemic), the picture is less clear - not because SDD causes harm, but because the baseline colonisation pressure likely overwhelms decontamination. Here, SOD alone - oropharyngeal paste without enteral antibiotics - may be the pragmatic middle ground.
The key variable clinicians underweight is surveillance. Units that adopt SDD without active weekly rectal and respiratory surveillance cultures cannot detect emerging resistance early. SDD without surveillance is not SDD as studied in the trials. Pair them or do neither.
A Frequently Overlooked Point: The Gastroenterologist's Role in SDD Decisions
Gastroenterologists are often asked to consult on ICU patients with gut dysfunction, altered motility, or concerns about enteral feeding - exactly the patients for whom the enteral component of SDD raises questions. What tends to be missed is that enteral SDD does not require normal gut motility to be effective. The non-absorbable antibiotics act locally on luminal flora; even with delayed gastric emptying or ileus, some decontamination effect persists. The more important gut-related consideration is fungal overgrowth: the amphotericin B component specifically targets Candida translocation, which is relevant in patients on prolonged antibiotics or with intestinal barrier failure. Removing it from the regimen - as some modified protocols do - sacrifices a pharmacologically justified component without clear benefit.
Bottom Line for Clinical Practice
SDD reduces ICU mortality and VAP with posterior probability >95% in Bayesian analyses - the evidence base is stronger than clinical adoption reflects.
Antibiotic resistance concerns are real but overweighted - trial data from low-to-moderate resistance settings show no measurable increase in resistant organism carriage with properly implemented SDD.
In high ESBL/carbapenem-resistance settings, consider SOD (oropharyngeal decontamination only) as a lower-resistance-footprint alternative that retains meaningful VAP reduction.
Active weekly surveillance cultures are mandatory - SDD without surveillance is not the intervention shown to be effective in RCTs.
The amphotericin B component should not be casually dropped - fungal decontamination is mechanistically justified, particularly in high-risk gut-dysfunction patients.
The next time an SDD question comes up on your ICU round or in a complex critically ill GI patient, bring the clinical details to GastroAGI - it will walk through the resistance context, patient profile, and current evidence to help you make a reasoned, individualised decision in real time.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.