13/05/2026
13viewsH. pylori Treatment in 2026: Choosing the Right First-Line Regimen When Clarithromycin Is No Longer the Default
The 2026 ACG guideline recommends BQT or vonoprazan-based therapy over PPI triple therapy for H. pylori. Here's how to choose between them.
Quick Answer
The 2026 ACG guideline recommends BQT or vonoprazan-based therapy over PPI triple therapy for H. pylori.
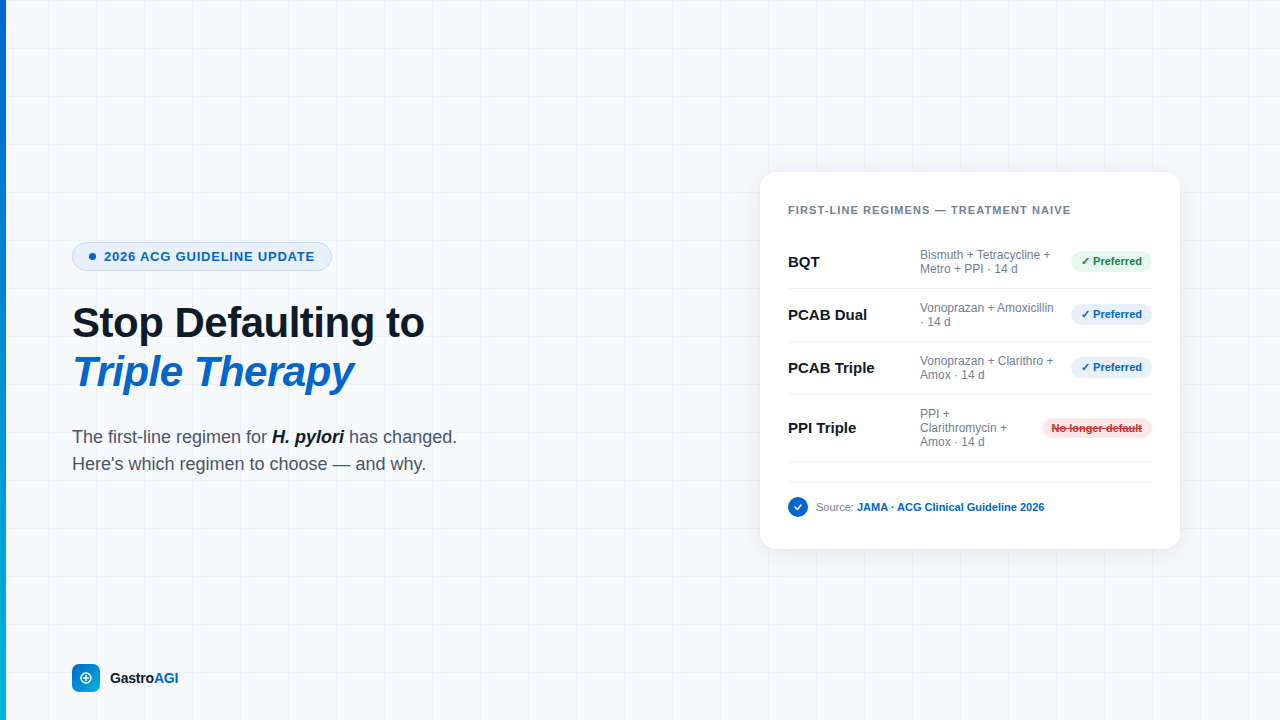
Your patient tests positive for H. pylori - straightforward PPI + clarithromycin + amoxicillin, right? Not anymore. Clarithromycin resistance has crossed 15–20% in most urban centres, and PPI triple therapy now fails in roughly one in four patients before you even factor in CYP2C19 metabolism. The 2026 ACG guideline has moved the goalposts on first-line treatment, and if you're still reaching for the old triple automatically, this post is for you.
The clinical problem isn't diagnosing H. pylori - it's eradicating it on the first attempt. Each failed treatment course selects for resistance, narrows your future options, and increases the patient's cumulative antibiotic exposure. The 2026 ACG Clinical Guideline (summarised in the March 2026 edition of JAMA) marks a decisive shift: PPI triple therapy is no longer the preferred first-line option except in specific, guideline-defined circumstances. The new defaults are bismuth quadruple therapy (BQT) and vonoprazan (PCAB)-based regimens - both achieving eradication rates above 85–90% even in the setting of clarithromycin resistance. Understanding when to use each, and why the old approach underperforms, is now a core competency for any clinician managing upper GI disease.
Why Bismuth Quadruple Therapy Has Become the Standard First-Line Approach
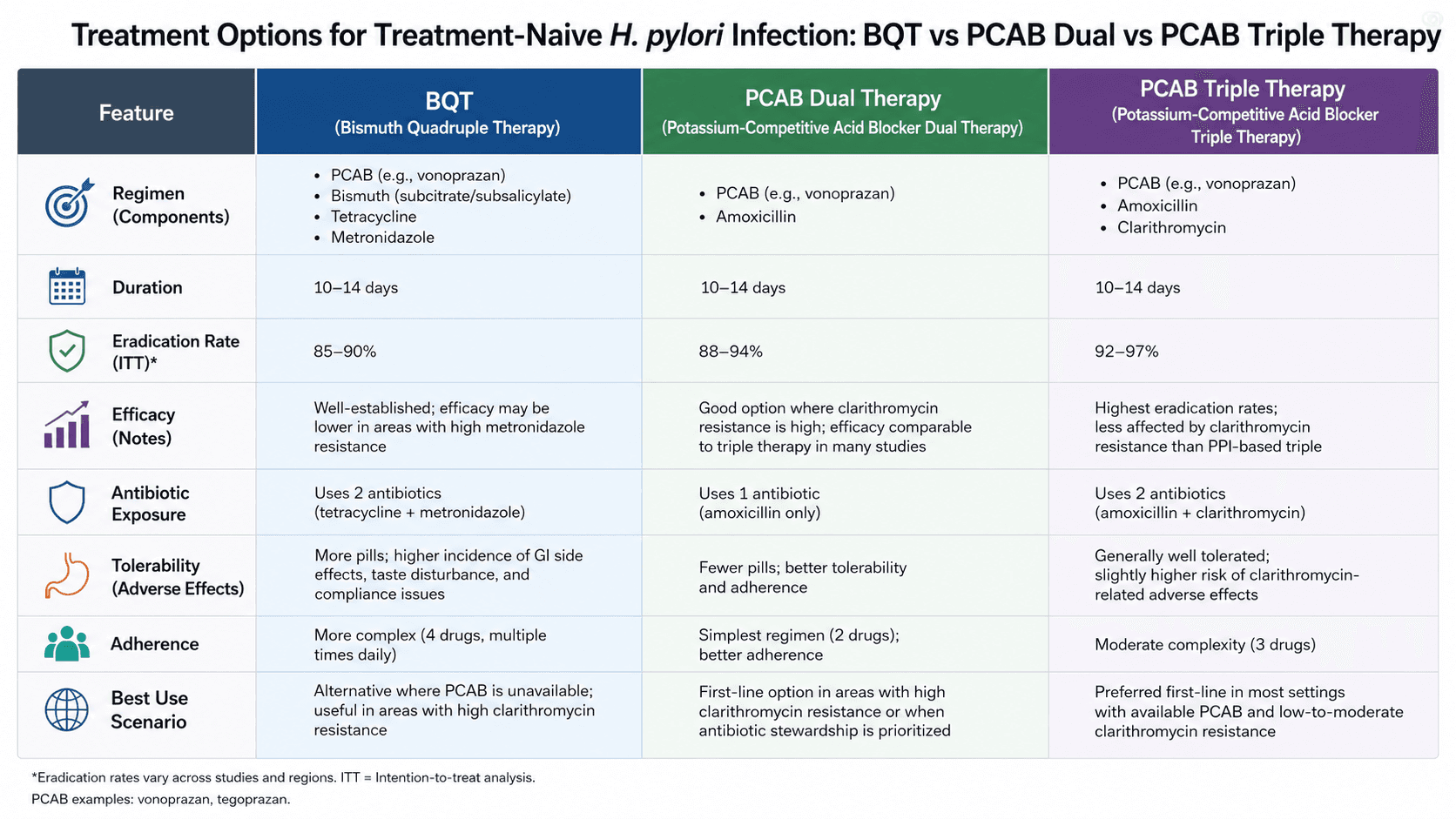
BQT - a PPI twice daily plus bismuth subcitrate (120–300 mg) or subsalicylate (300 mg) four times daily, tetracycline (500 mg) four times daily, and metronidazole (500 mg) three or four times daily for 14 days - achieves eradication rates of 85–95% in treatment-naive patients regardless of clarithromycin or metronidazole resistance status. This is the key point: BQT does not depend on clarithromycin sensitivity. Bismuth exerts a direct bactericidal effect on H. pylori at the mucosal surface, independent of antibiotic susceptibility testing, which is why it outperforms PPI triple therapy across resistance profiles.
Per the 2026 ACG guideline, BQT is recommended as a preferred first-line regimen for treatment-naive patients in the United States, where clarithromycin resistance rates exceed the 15% threshold that consistently degrades triple therapy outcomes. The 14-day course is not optional - shorter durations reduce eradication rates by 5–10 percentage points. The practical barrier is pill burden: patients take 14–16 tablets daily, which requires explicit counselling upfront. Adherence, not drug potency, becomes the rate-limiting factor. Set expectations at the first prescription: explain the schedule, name the likely side effects (bismuth black stools, mild nausea), and confirm there's no penicillin allergy before prescribing amoxicillin in any multi-drug regimen.
One secondary consideration worth noting: tetracycline resistance in H. pylori is rare globally, making BQT remarkably durable even as other antibiotic resistance patterns shift. In the absence of local susceptibility data - the reality for most outpatient gastroenterology practices - BQT is the most defensible empirical choice.
Clinical Scenario
A 38-year-old woman presents with a 4-month history of epigastric pain and early satiety. Endoscopy reveals a non-bleeding duodenal ulcer; rapid urease test is positive for H. pylori. She has no known drug allergies. Her GP had previously prescribed a 7-day PPI triple therapy course two years ago for "gastritis," and she reports she completed it - but was never tested for eradication.
Treatment with BQT (bismuth subcitrate 240 mg four times daily, tetracycline 500 mg four times daily, metronidazole 500 mg four times daily, omeprazole 20 mg twice daily) was initiated for 14 days. Urea breath test at 6 weeks post-treatment confirmed eradication. The clinical lesson here isn't just about regimen selection - it's about recognising prior treatment as a resistance risk factor. A patient with a previous failed or unconfirmed course should not receive PPI triple therapy empirically. BQT or susceptibility-guided therapy is the appropriate choice, and test-of-cure is mandatory after any eradication attempt.
Vonoprazan-Based Regimens: Where They Fit and When to Choose Them
Vonoprazan (a potassium-competitive acid blocker, or PCAB) represents a genuinely new mechanism in H. pylori treatment. Unlike PPIs, vonoprazan achieves near-complete acid suppression within hours and maintains it irrespective of CYP2C19 genotype - the pharmacokinetic variability that explains why "slow metabolisers" tolerate PPIs well but "rapid metabolisers" produce insufficient acid suppression and undermine antibiotic efficacy.
The 2026 ACG guideline endorses two vonoprazan-based regimens for treatment-naive patients:
PCAB dual therapy: Vonoprazan 20 mg twice daily + amoxicillin 1000 mg three times daily for 14 days
PCAB triple therapy: Vonoprazan 20 mg + clarithromycin 500 mg + amoxicillin 1000 mg twice daily for 14 days
PCAB dual therapy is particularly useful when metronidazole resistance is a concern or when minimising total antibiotic load is a priority. It delivers eradication rates of 80–87% in clinical trials, with a simpler dosing schedule than BQT. PCAB triple therapy performs comparably to BQT in clarithromycin-susceptible patients but loses its edge when clarithromycin resistance is present. The cost differential matters in many healthcare systems: vonoprazan is significantly more expensive than generic bismuth-tetracycline combinations, which may influence formulary decisions in resource-sensitive settings.
Rifabutin triple therapy (omeprazole 40 mg + amoxicillin 1000 mg + rifabutin 50 mg, all three times daily for 14 days) remains a guideline-endorsed option - particularly relevant for patients with penicillin intolerance requiring alternative backbones - but its use should be weighed against the risk of Mycobacterium resistance given rifabutin's role in TB regimens.
A Frequently Overlooked Point: Test-of-Cure Is Not Optional
The most common gap in H. pylori management in clinical practice is not regimen selection - it's the failure to confirm eradication. The 2026 ACG guideline and prior ACG/AGA consensus are explicit: all patients treated for H. pylori should undergo test-of-cure at least 4 weeks after completing antibiotics and at least 2 weeks after stopping PPIs. The urea breath test and stool antigen test are both acceptable; serology is not. In patients with peptic ulcer disease or a family history of gastric cancer, eradication confirmation is not a courtesy - it is the clinical endpoint. Missing this step leaves you with a patient who believes they've been treated while carrying viable, now-resistant H. pylori, and a chart that offers no guidance when they return symptomatic in 18 months.
Bottom Line for Clinical Practice
Stop defaulting to PPI triple therapy as empirical first-line treatment. Clarithromycin resistance rates in most urban populations now exceed the 15% threshold below which triple therapy is defensible.
BQT for 14 days is the most robust empirical regimen for treatment-naive patients - resistance-independent and well-validated across populations.
Vonoprazan dual or triple therapy is a guideline-endorsed alternative with simpler dosing; particularly useful when CYP2C19 variability or metronidazole resistance is a concern.
Any prior treatment course, even one claimed to be completed, should prompt susceptibility-guided therapy or a switch to BQT - not re-prescription of triple therapy.
Confirm eradication with UBT or stool antigen at least 4 weeks post-antibiotics and 2 weeks post-PPI in every patient, without exception.
The next time you're standing at the prescription pad deciding between these regimens, walk GastroAGI through the case - prior treatment history, allergy status, local resistance patterns - and get a guideline-anchored recommendation in seconds. And if you're managing H. pylori in an Indian clinical context, read our deep-dive on H. pylori Treatment Guidelines in India - local resistance data, regimen availability, and what the evidence actually supports in your practice setting.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.