20/05/2026
6viewsObesity is Plateauing in the West and Accelerating Everywhere Else: What That Means for Clinical Practice
Obesity is still accelerating in 100+ countries. Where undernutrition persists alongside it, standard bariatric approaches fall short. Here's what evidence supports.
Quick Answer
Obesity is still accelerating in 100+ countries. Where undernutrition persists alongside it, standard bariatric approaches fall short.
A 34-year-old woman from a Pacific Island nation presents with a BMI of 38, type 2 diabetes diagnosed two years ago, and a haemoglobin of 9.4 g/dL. She has visible signs of iron and B12 deficiency alongside frank visceral obesity. She is, in nutritional terms, both overnourished and undernourished simultaneously. This is not an edge case anymore - it is the clinical reality of obesity in 2026 across much of the low- and middle-income world, and treating only one half of the picture will fail the patient.
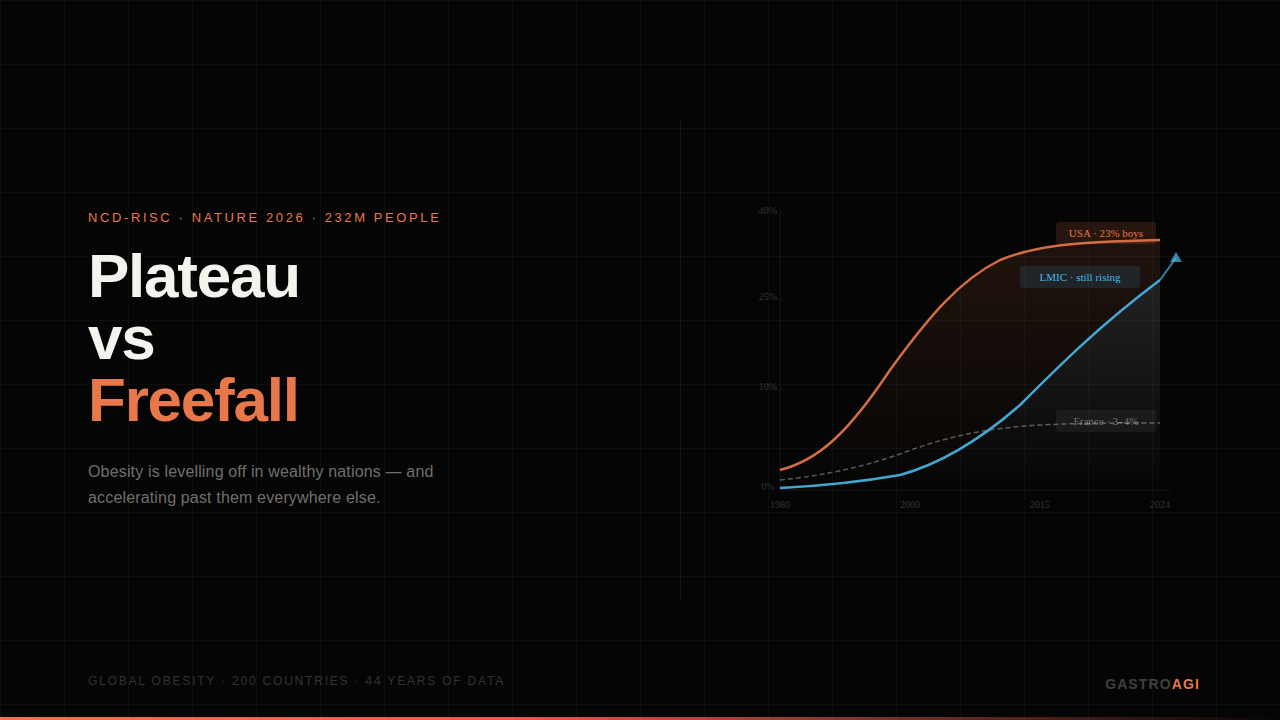
The largest epidemiological analysis of obesity ever published - the NCD Risk Factor Collaboration's 2026 study in Nature, tracking 232 million individuals across 200 countries from 1980 to 2024 - does not just tell us where obesity is. It tells us how fast it is moving, and which populations are now past the inflection point. The findings have direct implications for how gastroenterologists and GI clinicians approach obesity-related disease in patients coming from different epidemiological backgrounds.
The Velocity Data Changes the Conversation on Global Obesity Acceleration
Prevalence statistics are a snapshot. Velocity - the year-on-year rate of change - is the leading indicator, and the NCD-RisC analysis treated it as the primary signal.
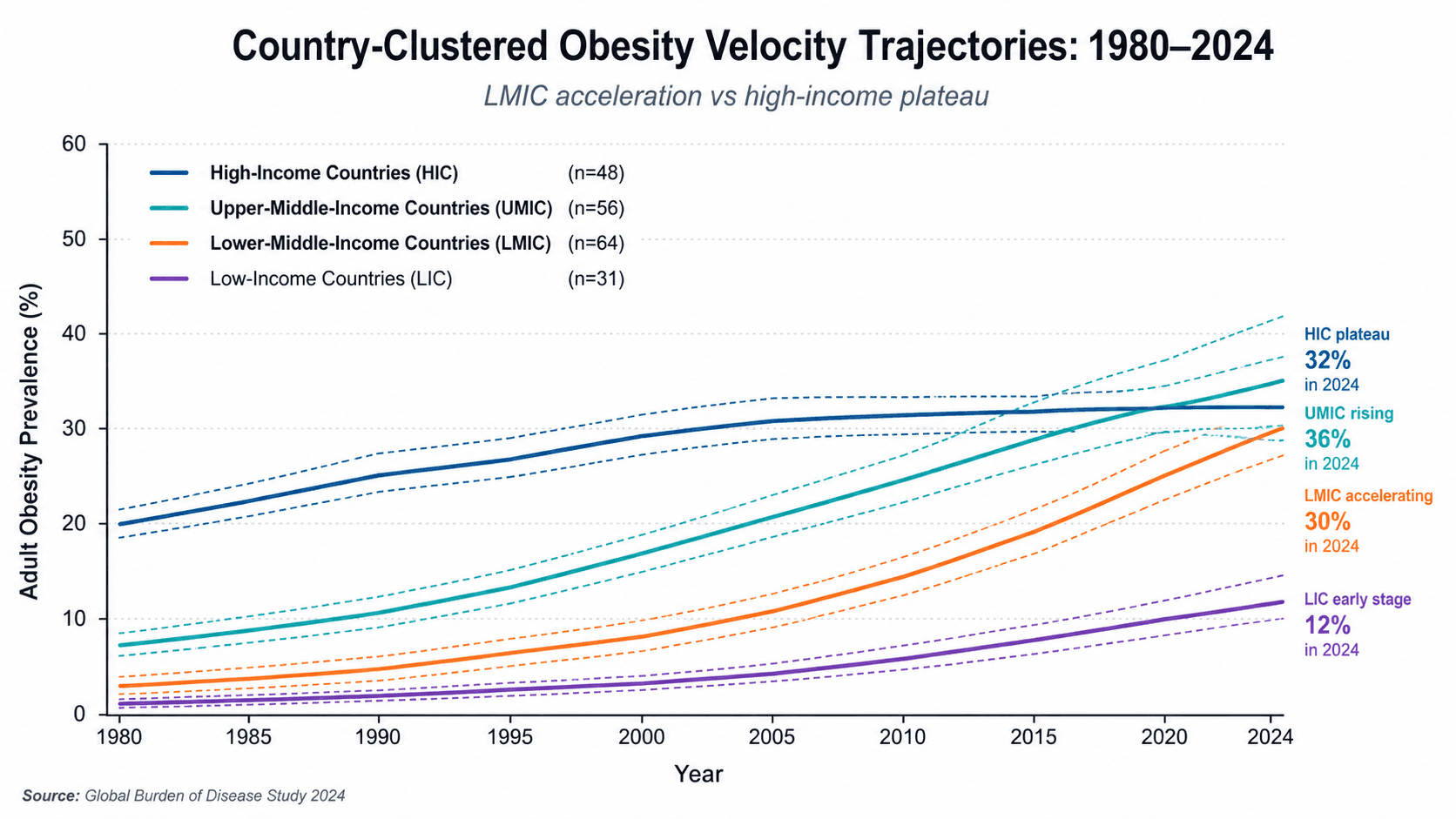
In high-income Western nations, the story is essentially one of early alarms followed by a slow ceiling. The rise in childhood obesity began decelerating around 1990 and plateaued in most of these countries by the mid-2000s. Adults followed roughly a decade behind. Importantly, these plateaus do not represent the same level of harm. Girls in Japan, Denmark, and France plateaued at a childhood obesity prevalence of 3–4%. Boys in the United States plateaued at 23%. Adult prevalence among "plateaued" nations ranges from 11% in France to 25–43% in the UK, Canada, and the United States. A plateau is not a solution - it is a permanently elevated baseline from which metabolic disease, MASLD, and GI malignancy will continue accumulating for decades.
In low- and middle-income countries (LMICs), the curve is still climbing. As of 2024, obesity prevalence was rising at more than 0.5 percentage points per year in 100 countries for women and 66 countries for men. The steepest accelerations are in Pacific Island nations, sub-Saharan Africa, and parts of South and Southeast Asia. Several of these trajectories have already surpassed the peak velocities ever recorded in the West. Per the NCD-RisC analysis, this is not simply the West's obesity story playing out on a time delay - the social and nutritional contexts are structurally different, which changes how the disease presents and how it should be managed.
Clinical Scenario: The Dual-Burden Patient Who Doesn't Fit Standard Algorithms
A 41-year-old man from a semi-urban area of sub-Saharan Africa presents to a tertiary centre with MASLD confirmed on fibroscan (liver stiffness 9.8 kPa), a BMI of 33, and a random blood glucose of 14.2 mmol/L. His dietary history reveals high refined carbohydrate intake, low protein, and near-zero dietary fat - not excess calories across the board, but a severe macronutrient imbalance. His albumin is 29 g/L. He has not eaten animal protein more than twice weekly throughout his life.
Applying standard MASLD or obesity management guidelines - designed around a well-nourished, sedentary, calorically-replete Western patient - produced a recommendation for caloric restriction and a referral pathway toward GLP-1 therapy. The caloric restriction, without correcting protein and micronutrient deficiency first, worsened his sarcopenia and delayed glycaemic improvement. The clinical team course-corrected only after a dietitian flagged his MUAC and the discrepancy between his visceral fat burden and his lean mass. The case is a reminder that obesity management algorithms embedded in GI practice were not derived from patients carrying a simultaneous undernutrition burden.
Managing Obesity Where Undernutrition Persists: What the Evidence Supports
The dual burden of malnutrition - obesity coexisting with micronutrient deficiency and/or protein-energy undernutrition - is now formally recognised by the WHO and FAO as a distinct nutritional phenotype, most common in urban populations in LMICs undergoing rapid dietary transition. For gastroenterologists, this matters in at least three clinical scenarios: pre-bariatric surgery assessment, MASLD management, and nutritional rehabilitation after GI illness.
In bariatric surgery candidates from high-velocity obesity regions, pre-operative nutritional assessment needs to go beyond BMI and standard metabolic panels. Thiamine, iron, folate, B12, zinc, and vitamin D deficiencies are prevalent at baseline in LMIC populations seeking bariatric intervention - and post-surgical malabsorption compounds what is already an under-repleted reserve. A 2023 systematic review in Obesity Reviews found that pre-operative micronutrient deficiency rates in LMICs were consistently two to three times higher than in matched Western bariatric cohorts. This is not a contraindication to surgery; it is an argument for a minimum 3-month nutritional optimisation window before any bariatric procedure, and for extending post-operative supplementation protocols.
In MASLD, the dual-burden phenotype often presents with a pattern of hepatic steatosis without the dyslipidaemia pattern typical of Western patients. Triglycerides may be near-normal; LDL unremarkable. The driver is hyperinsulinaemia from refined carbohydrate load combined with insufficient dietary protein to support hepatic lipid export. Management here prioritises protein adequacy and glycaemic index modification over aggregate caloric reduction - a subtle but important distinction from standard MASLD dietary guidance.
Where GLP-1 receptor agonists are unavailable or unaffordable - which describes most of the 100 countries still in the obesity acceleration phase - realistic interventions lean on dietary modification, structured physical activity, and treating the undernutrition component as a prerequisite rather than an afterthought. The evidence base for metformin as an adjunct in this population remains robust and affordable.
A Frequently Overlooked Point: "Plateau" Does Not Mean Harm Has Stopped
There is a tendency in clinical practice to view plateaued obesity prevalence in high-income countries as a policy success story. The NCD-RisC data complicates this. A plateau at 40% adult obesity - as in the United States - still means a relentlessly expanding pool of patients with MASLD, cirrhosis, oesophageal adenocarcinoma, and colorectal cancer. The lag between obesity prevalence and GI malignancy incidence runs to 10–20 years. Countries that plateaued in the early 2000s are now entering the peak period for those downstream consequences. Gastroenterologists in both plateaued and accelerating countries will be managing more obesity-attributable GI disease, not less, for the next two decades regardless of what prevention programmes achieve.
Bottom Line for Clinical Practice
Screen dual-burden nutritional status explicitly in any obese patient from a high-velocity obesity region or LMIC background - do not assume obesity equals nutritional sufficiency. Albumin, MUAC, and a targeted micronutrient panel (thiamine, B12, iron, zinc, D) should be standard.
Pre-bariatric nutritional optimisation matters more, not less, in LMIC-origin patients - a minimum 3-month correction window for identified deficiencies before surgery, with extended post-operative supplementation protocols.
In MASLD with dual-burden phenotype, prioritise protein adequacy and glycaemic index reduction over aggregate caloric restriction; the steatosis driver is macronutrient imbalance, not pure caloric excess.
Plateau in high-income countries does not reduce GI disease burden - the lag between obesity prevalence and downstream GI malignancy means colonoscopy demand, MASLD progression cases, and oesophageal cancer referrals will continue rising in plateaued nations well into the 2030s.
Where GLP-1 agents are unavailable, structured dietary protein rehabilitation combined with metformin and glycaemic index-targeted dietary advice represents the most evidence-supported accessible pathway for the dual-burden obese patient.
When a case like this lands in front of you - obesity with concurrent nutritional deficiency, an atypical MASLD lipid profile, or a pre-bariatric patient from a high-velocity obesity region - walk GastroAGI through the clinical details. It will apply the relevant nutritional and GI evidence to your specific patient, not the textbook average.
Read More on: Obesity Pharmacotherapy in 2026: How EASO's Complication-First Framework Changes the Way You Choose a Drug
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.