25/05/2026
12viewsFIB-4 in MASLD: When to Trust It, When It Fails, and What to Do in the Grey Zone
FIB-4 misses advanced fibrosis in MASLD patients with diabetes or obesity. Here's when to trust it, when it fails, and what to do next.
Quick Answer
FIB-4 misses advanced fibrosis in MASLD patients with diabetes or obesity. Here's when to trust it, when it fails, and what to do next.
Your patient is a 54-year-old woman with type 2 diabetes, a BMI of 33, and incidentally detected hepatic steatosis on abdominal ultrasound. You calculate her FIB-4 - it comes back at 1.1, which puts her in the low-risk category. You file it, reassure her, and plan a repeat in a year. Two years later she re-presents with fatigue and a platelet count of 118. Her FibroScan shows liver stiffness of 11.2 kPa. She has bridging fibrosis. The FIB-4 missed it. This post explains exactly why, and what your workup should have looked like.
FIB-4 MASLD liver fibrosis staging has become the default first step in most outpatient referral pathways - and for good reason. It uses four variables you already have (age, AST, ALT, platelet count), requires no imaging, costs nothing, and carries guideline endorsement from both the AGA and EASL. The March 2026 AGA Clinical Care Pathway for MASLD explicitly recommends FIB-4 as the first-line tool to stratify fibrosis risk in at-risk patients before any further investigation. That guidance is sound in broad populations. The problem is that the patients who land in your clinic are rarely a broad population. They are diabetic, obese, older, or all three - and that is precisely where FIB-4's diagnostic performance degrades in ways the standard thresholds do not warn you about.
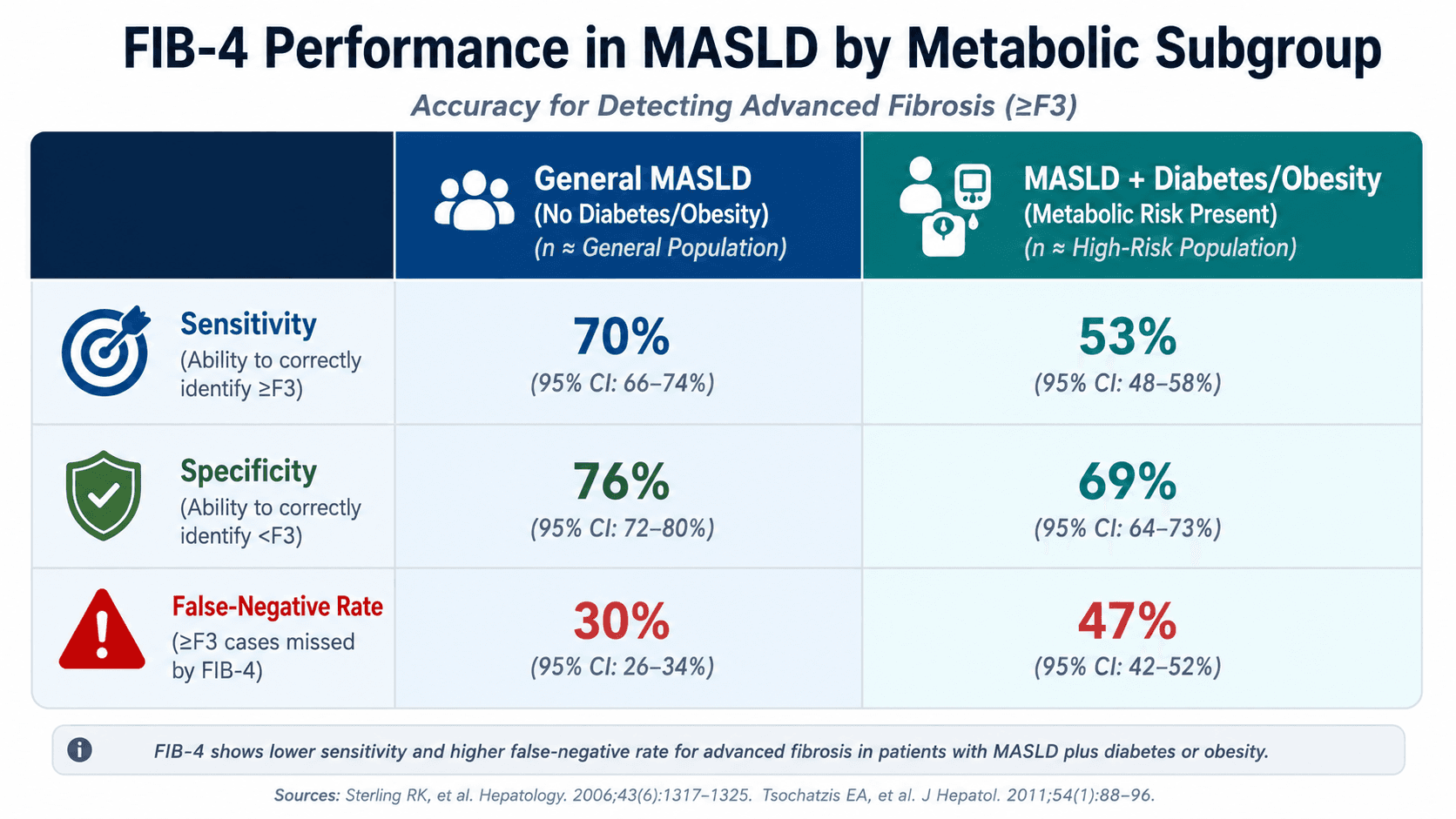
A January 2026 paper in JHEP Reports, drawing from primary care MASLD cohorts in Belgium and the Netherlands, demonstrated that FIB-4 systematically under-triages patients with type 2 diabetes or BMI ≥30, even when the score falls below the 1.30 threshold typically used to exclude significant fibrosis. In other words, a score that should be reassuring is not, in the metabolic patients who make up the majority of your MASLD caseload. Understanding where FIB-4 breaks down - and how to navigate that grey zone - is now a core clinical competency, not an optional nuance.
What FIB-4 Actually Measures - and Where the Thresholds Come From
FIB-4 was originally validated in HIV/HCV co-infected patients in 2006, then adopted broadly across chronic liver disease. Its formula - (age × AST) / (platelet count × √ALT) - is a surrogate for portal hypertension-associated platelet destruction and hepatocyte injury. It performs reliably at the extremes: a score below 1.30 has a high negative predictive value for advanced fibrosis in general MASLD populations, and a score above 2.67 carries high specificity for significant fibrosis. The indeterminate zone between 1.30 and 2.67 is where most clinical decisions stall.
What the validation studies cannot fix is a structural issue: FIB-4 is not fibrosis-specific. It reflects the metabolic and inflammatory milieu as much as the fibrotic burden. In patients with type 2 diabetes, chronically elevated AST from insulin resistance inflates the numerator independently of fibrosis stage. In obese patients, thrombocytosis from the pro-inflammatory state artificially suppresses the score by boosting the denominator. Both effects push the result toward the low-risk range even when the liver is accumulating collagen at F2 or F3 stage. A meta-analysis published in the International Journal of Hepatology in 2026, analysing 14 studies across 5,521 MASLD patients, found that FIB-4 at the standard 1.30 cut-off missed a clinically significant proportion of advanced fibrosis cases - with accuracy declining further in cohorts with higher rates of diabetes and obesity. This is not a fringe finding. It is a systematic limitation that applies directly to the patients most likely to progress.
Clinical Scenario
A 61-year-old man with a 12-year history of type 2 diabetes and a BMI of 34 is referred from his GP after an ultrasound reports moderate hepatic steatosis. His liver enzymes are mildly elevated - ALT 52 U/L, AST 41 U/L. Platelet count is 196 × 10⁹/L. FIB-4 calculates to 1.18. Standard pathway would classify him as low risk and discharge back to primary care with annual monitoring.
Instead, recognising his dual metabolic risk flags - diabetes and obesity, both documented FIB-4 confounders - you refer him for vibration-controlled transient elastography (VCTE). His liver stiffness measurement comes back at 9.4 kPa, consistent with F3 fibrosis. CAP score confirms significant steatosis. He is referred for hepatology input, commenced on lifestyle intervention, and enrolled in a GLP-1 trial. Without the elastography step, this patient's bridging fibrosis would have been missed for at least another year - the window where antifibrotic intervention has the most impact.
What to Do When FIB-4 Falls in the Low or Indeterminate Range but Risk Factors Are High
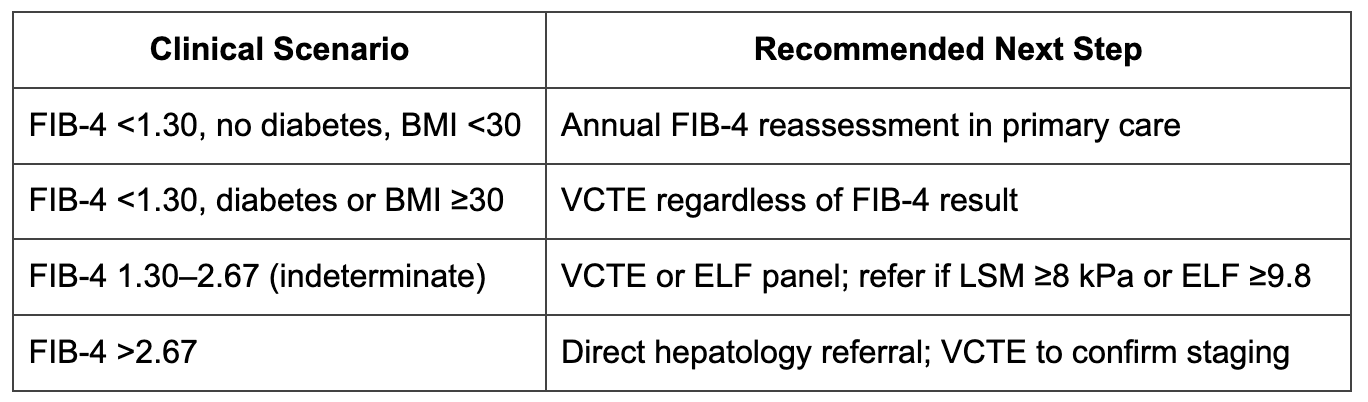
The 2026 JHEP Reports data provide a practical rule that is not yet embedded in most referral guidelines: in patients with MASLD plus diabetes or BMI ≥30, do not use a FIB-4 below 1.30 as a standalone rule-out for significant fibrosis. These patients warrant second-line non-invasive fibrosis assessment regardless of the FIB-4 result.
The preferred second-line tool in most settings is VCTE (FibroScan). A liver stiffness measurement below 8 kPa in a fasted, adequately windowed patient provides reliable exclusion of F3–F4 fibrosis. Above 8 kPa - or where VCTE is unavailable or technically limited by BMI - MR elastography offers superior accuracy and is increasingly accessible at tertiary centres. For clinical settings where elastography access is limited, the Enhanced Liver Fibrosis (ELF) panel is an evidence-based serum alternative; an ELF score ≥9.8 should trigger liver specialist referral regardless of FIB-4 result.
Liver biopsy remains the reference standard when non-invasive tests conflict, when the clinical picture suggests a competing aetiology contributing to fibrosis acceleration (alcohol, metabolic syndrome combined with viral hepatitis, drug-induced injury), or when treatment-trial eligibility requires histological staging. When to biopsy MASLD is not a binary question driven by FIB-4 alone - it is a sequential decision that accounts for the full metabolic profile. For an updated take on what happens once staging confirms MASH with fibrosis, see GastroAGI's deep-dive on sequencing resmetirom and GLP-1 therapy in confirmed MASH with fibrosis.
A Frequently Overlooked Point: Age Inflates FIB-4 Without Reflecting True Fibrosis Burden
Clinicians rarely scrutinise the age term in the FIB-4 formula, but they should. Because age multiplies directly against AST in the numerator, an older patient with even mildly elevated transaminases will generate a higher FIB-4 score regardless of fibrotic activity. The converse is equally important: in younger patients - those under 35 with early MASLD - FIB-4 frequently underestimates fibrosis because a low age term deflates the score even when hepatic inflammation is active. Both groups warrant elastography-based confirmation rather than reliance on FIB-4 at face value. The score was not designed to be age-agnostic, and managing it as if it were produces predictable misclassifications at both ends of the age spectrum.
Bottom Line for Clinical Practice
Do not use FIB-4 <1.30 as a standalone rule-out in MASLD patients with type 2 diabetes or BMI ≥30 - the false-negative rate in this subgroup is clinically unacceptable. Proceed to VCTE.
VCTE threshold of 8 kPa is the practical trigger for specialist referral in patients with indeterminate or falsely reassuring FIB-4; above this threshold, F3+ fibrosis is likely.
The indeterminate zone (FIB-4 1.30–2.67) should always prompt second-line testing - it is not a safe holding category, particularly in older or diabetic patients.
ELF ≥9.8 warrants hepatology referral even if FIB-4 is low, particularly where VCTE is unavailable or technically limited. If that referral reveals decompensated disease, the GastroAGI guide on managing decompensated cirrhosis once fibrosis progresses covers the next decision layer.
Liver biopsy is not the answer to every diagnostic question in MASLD, but it remains essential when non-invasive tests conflict, competing aetiologies are present, or treatment-trial enrolment requires histological staging. If advanced disease is confirmed and the patient deteriorates acutely, the framework fordistinguishing ACLF from ALF when the patient deteriorates becomes the relevant next step.
The next time a MASLD patient with diabetes or significant obesity comes back with a FIB-4 score that puts you at ease, pause before filing it. The score may be right - or it may be hiding bridging fibrosis in the one patient subgroup where it consistently underperforms. Walk GastroAGI through the clinical details - age, metabolic comorbidities, FIB-4 result, VCTE availability - and get a structured, guideline-anchored next-step recommendation in seconds.
We are pioneers in clinical intelligence, dedicated to helping gastroenterologists harness the power of artificial intelligence to drive precision, efficiency, and patient growth.